

Defining geriatric trauma: when does age make a difference?
- PMID: 23021136
- PMCID: PMC4070315
- DOI: 10.1016/j.surg.2012.08.017
Defining geriatric trauma: when does age make a difference?
Abstract
Background: Injured elderly patients experience high rates of undertriage to trauma centers (TCs) whereas debate continues regarding the age defining a geriatric trauma patient. We sought to identify when mortality risk increases in injured patients as the result of age alone to determine whether TC care was associated with improved outcomes for these patients and to estimate the added admissions burden to TCs using an age threshold for triage.
Methods: We performed a retrospective cohort study of injured patients treated at TCs and non-TCs in Pennsylvania from April 1, 2001, to March 31, 2005. Patients were included if they were between 19 and 100 years of age and had sustained minimal injury (Injury Severity Score < 9). The primary outcome was in-hospital mortality. We analyzed age as a predictor of mortality by using the fractional polynomial method.
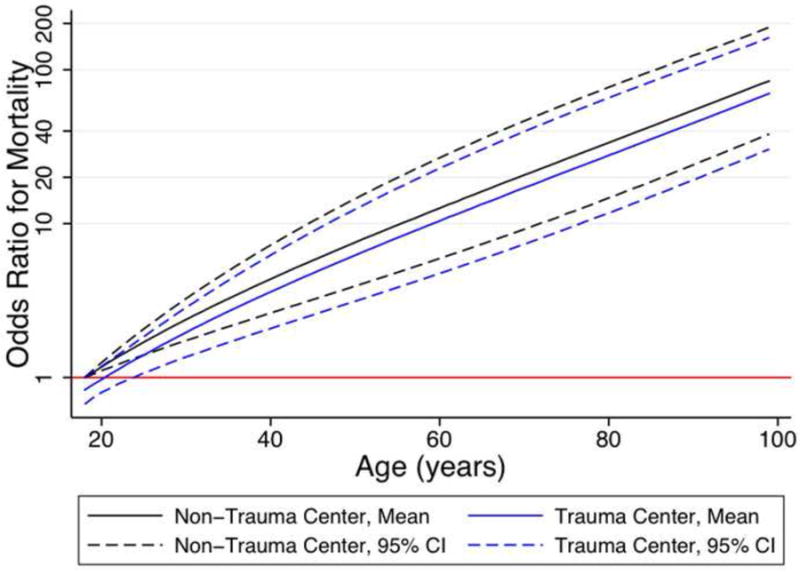
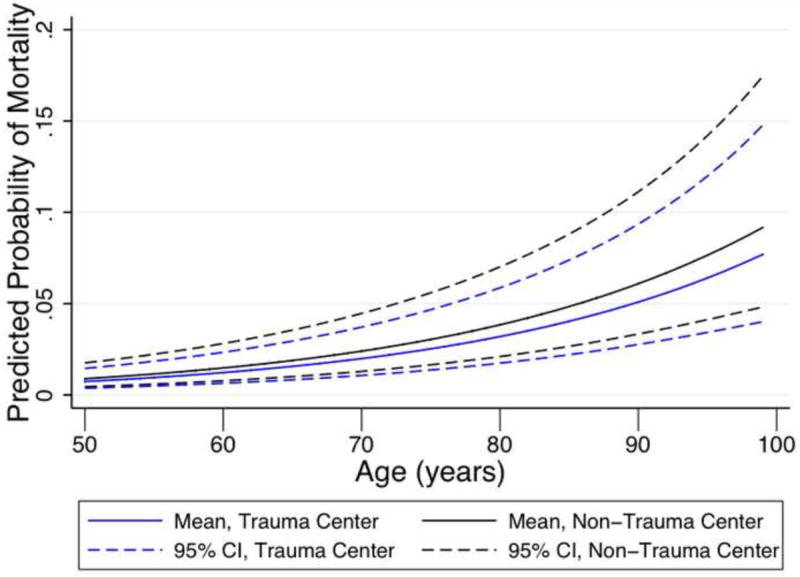
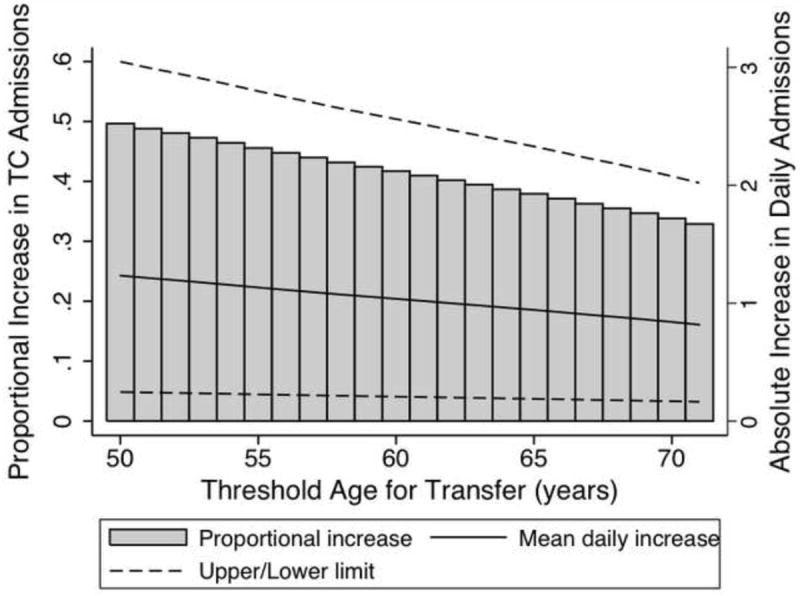
Results: A total of 104,015 patients were included. Mortality risk significantly increased at 57 years (odds ratio 5.58; 95% confidence interval 1.07-29.0; P = .04) relative to 19-year-old patients. TC care was associated with a decreased mortality risk compared with non-TC care (odds ratio 0.83; 95% confidence interval 0.69-0.99; P = .04). Using an age of 70 as a threshold for mandatory triage, we estimated TCs could expect an annual increase of approximately one additional admission per day.
Conclusion: Age is a significant risk factor for mortality in trauma patients, and TC care improves outcomes even in older, minimally injured patients. An age threshold should be considered as a criterion for TC triage. Use of the clinically relevant age of 70 as this threshold would not impose a substantial increase on annual TC admissions.
Copyright © 2012 Mosby, Inc. All rights reserved.
Figures

References
-
- Minino AM, Xu J, Kochanek KD, Tejada-Vera B. Death in the United States, 2007. NCHS data brief. 2009 Dec;(26):1–8. - PubMed
-
- MacKenzie EJ, Rivara FP, Jurkovich GJ, et al. A national evaluation of the effect of trauma-center care on mortality. The New England journal of medicine. 2006 Jan 26;354(4):366–378. - PubMed
-
- Ma MH, MacKenzie EJ, Alcorta R, Kelen GD. Compliance with prehospital triage protocols for major trauma patients. The Journal of trauma. 1999 Jan;46(1):168–175. - PubMed
-
- Chang DC, Bass RR, Cornwell EE, Mackenzie EJ. Undertriage of elderly trauma patients to state-designated trauma centers. Arch Surg. 2008 Aug;143(8):776–781. discussion 782. - PubMed
-
- Phillips S, Rond PC, 3rd, Kelly SM, Swartz PD. The failure of triage criteria to identify geriatric patients with trauma: results from the Florida Trauma Triage Study. The Journal of trauma. 1996 Feb;40(2):278–283. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
