

The population burden of heart failure attributable to modifiable risk factors: the ARIC (Atherosclerosis Risk in Communities) study
- PMID: 23021327
- PMCID: PMC3653309
- DOI: 10.1016/j.jacc.2012.07.022
The population burden of heart failure attributable to modifiable risk factors: the ARIC (Atherosclerosis Risk in Communities) study
Abstract
Objectives: The goal of this study was to estimate the population burden of heart failure and the influence of modifiable risk factors.
Background: Heart failure is a common, costly, and fatal disorder, yet few studies have evaluated the population-level influence of modifiable risk factors.
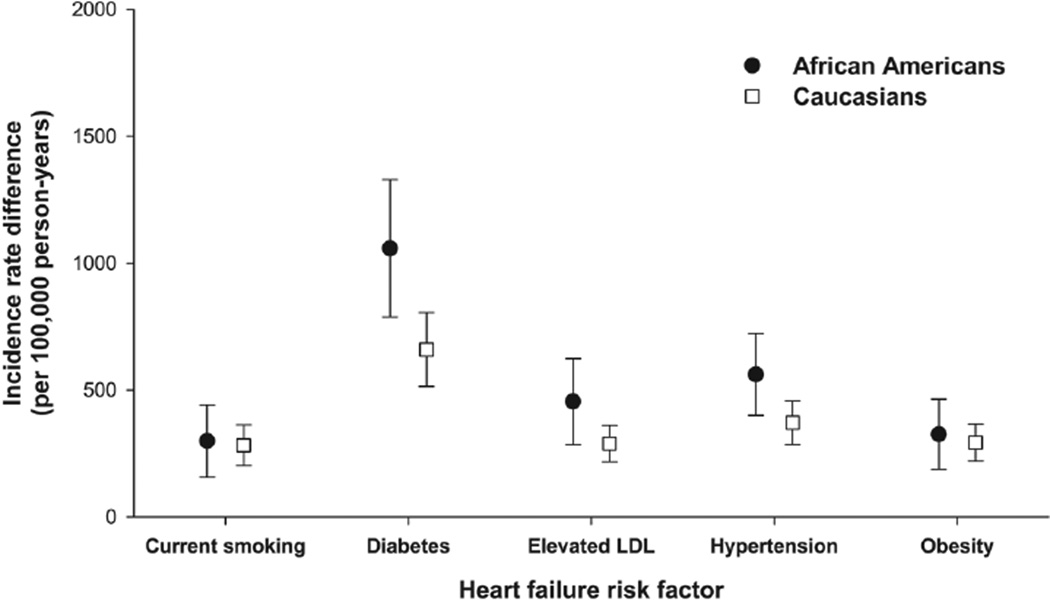
Methods: From 14,709 ARIC (Atherosclerosis Risk in Communities) study participants, we estimated incidence rate differences (IRD) for the association between 5 modifiable risk factors (cigarette smoking, diabetes, elevated low-density lipoproteins, hypertension, and obesity) and heart failure. Potential impact fractions were used to measure expected changes in the heart failure incidence assuming achievement of a 5% proportional decrement in the prevalence of each risk factor.
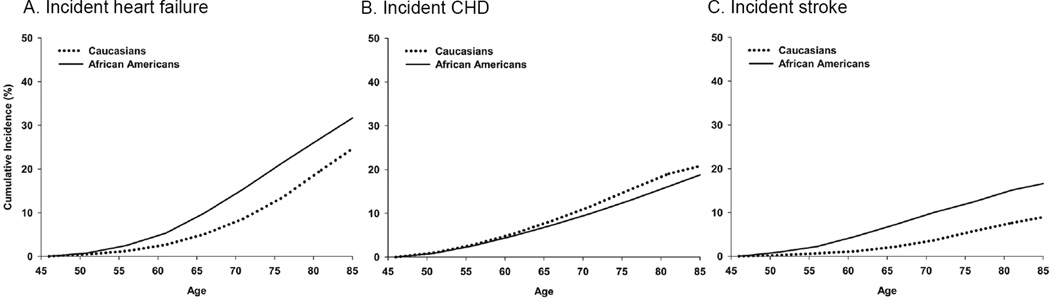
Results: Over an average of 17.6 years of follow-up, 1 in 3 African American and 1 in 4 Caucasian participants were hospitalized with heart failure, defined as the first hospitalization with International Classification of Diseases, Ninth Revision discharge codes of 428.x. Of the 5 modifiable risk factors, the largest IRD was observed for diabetes, which was associated with 1,058 (95% confidence interval [CI]: 787 to 1,329) and 660 (95% CI: 514 to 805) incident hospitalizations of heart failure/100,000 person-years among African-American and Caucasian participants, respectively. A 5% proportional reduction in the prevalence of diabetes would result in approximately 53 and 33 fewer incident heart failure hospitalizations per 100,000 person-years in African-American and Caucasian ARIC participants, respectively. When applied to U.S. populations, this reduction may prevent approximately 30,000 incident cases of heart failure annually.
Conclusions: Modest decrements in the prevalence of modifiable heart failure risk factors such as diabetes may substantially decrease the incidence of this major disease.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- American Heart Association. 2010 Heart and stroke statistical update. Dallas, TX: American Heart Association; 2010.
-
- Roger VL, Weston SA, Redfield MM, et al. Trends in heart failure incidence and survival in a community-based population. JAMA. 2004;292:344–350. - PubMed
-
- Kozak LJ, DeFrances CJ, Hall MJ. National hospital discharge survey: 2004 annual summary with detailed diagnosis and procedure data. Vital Health Stat. 2006;13:1–209. - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–1428. - PubMed
-
- SOLVD Investigators. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions, congestive heart failure The SOLVD Investigators. N Engl J Med. 1991;325:293–302. - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- R00-HL-098458/HL/NHLBI NIH HHS/United States
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- R00 HL098458/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
