

Prediction of mortality in clinical practice for medicare patients undergoing defibrillator implantation for primary prevention of sudden cardiac death
- PMID: 23021331
- PMCID: PMC3677038
- DOI: 10.1016/j.jacc.2012.07.028
Prediction of mortality in clinical practice for medicare patients undergoing defibrillator implantation for primary prevention of sudden cardiac death
Abstract
Objectives: The aim of this study was to derive and validate a practical risk model to predict death within 4 years of primary prevention implantable cardioverter-defibrillator (ICD) implantation.
Background: ICDs for the primary prevention of sudden cardiac death improve survival, but recent data suggest that a patient subset with high mortality and minimal ICD benefit may be identified.
Methods: Data from a development cohort (n = 17,991) and validation cohort (n = 27,893) of Medicare beneficiaries receiving primary prevention ICDs from 2005 to 2007 were merged with outcomes data through mid-2010 to construct and validate complete and abbreviated risk models for all-cause mortality using Cox proportional hazards regression.
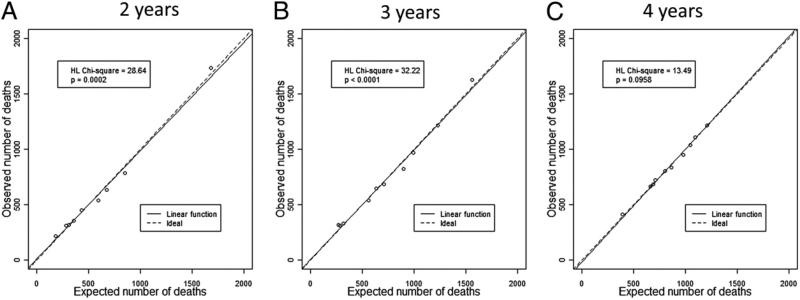
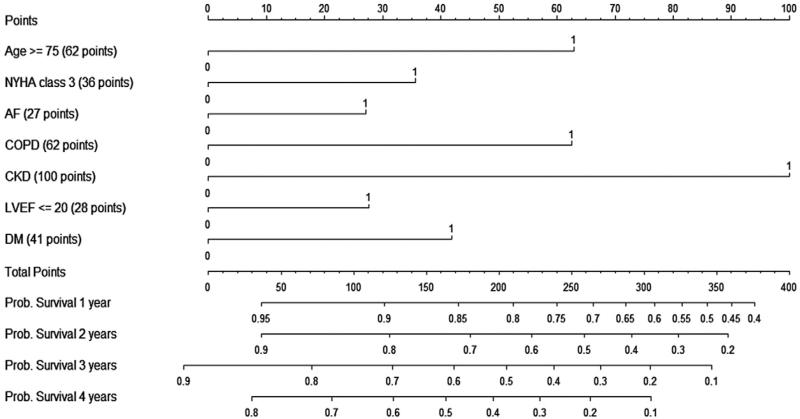
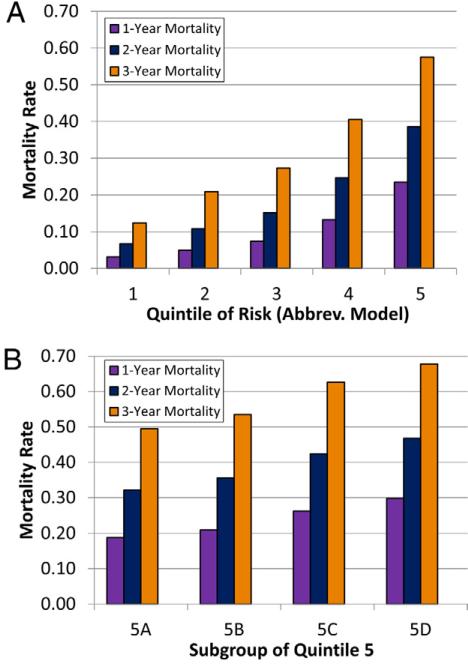
Results: Over a median follow-up period of 4 years, 6,741 (37.5%) development and 8,595 (30.8%) validation cohort patients died. The abbreviated model was based on 7 clinically relevant predictors of mortality identified from complete model results, referred to as the "SHOCKED" predictors: 75 years of age or older (hazard ratio [HR]: 1.70; 95% confidence interval [CI]: 1.62 to 1.79), heart failure (New York Heart Association functional class III) (HR: 1.35; 95% CI: 1.29 to 1.42), out of rhythm because of atrial fibrillation (HR: 1.26; 95% CI: 1.19 to 1.33), chronic obstructive pulmonary disease (HR: 1.70; 95% CI: 1.61 to 1.80), kidney disease (chronic) (HR: 2.33; 95% CI: 2.20 to 2.47), ejection fraction (left ventricular) ≤ 20% (HR: 1.26; 95% CI: 1.20 to 1.33), and diabetes mellitus (HR: 1.43; 95% CI: 1.36 to 1.50). This model had C-statistics of 0.75 (95% CI: 0.75 to 0.76) and 0.74 (95% CI: 0.74 to 0.75) in the development and validation cohorts, respectively. Validation patients in the highest risk decile on the basis of the SHOCKED predictors had a 65% 3-year mortality rate. A nomogram is provided for survival probabilities 1 to 4 years after ICD implantation.
Conclusions: This useful model, based on more than 45,000 primary prevention ICD patients, accurately identifies patients at highest risk for death after device implantation and may significantly influence clinical decision making.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Implantable cardioverter-defibrillators for primary prevention of sudden death: the quest to identify patients most likely to benefit.J Am Coll Cardiol. 2012 Oct 23;60(17):1656-8. doi: 10.1016/j.jacc.2012.06.041. Epub 2012 Sep 26. J Am Coll Cardiol. 2012. PMID: 23021332 No abstract available.
References
-
- Moss AJ, Hall WJ, Cannom DS, et al. for the Multicenter Automatic Defibrillator Implantation Trial Investigators Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. N Engl J Med. 1996;335:1933–40. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877–83. - PubMed
-
- Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–37. - PubMed
-
- Buxton AE, Lee KL, DiCarlo L, et al. for the Multicenter Unsustained Tachycardia Trial Investigators Electrophysiologic testing to identify patients with coronary artery disease who are at risk for sudden death. N Engl J Med. 2000;342:1937–45. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
