

Variability of ICU use in adult patients with minor traumatic intracranial hemorrhage
- PMID: 23021347
- PMCID: PMC3880139
- DOI: 10.1016/j.annemergmed.2012.08.024
Variability of ICU use in adult patients with minor traumatic intracranial hemorrhage
Abstract
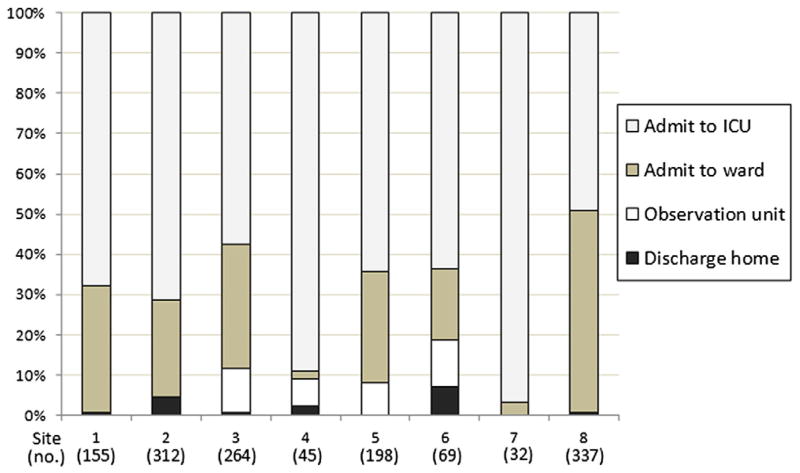
Study objective: Patients with minor traumatic intracranial hemorrhage are frequently admitted to the ICU, although many never require critical care interventions. To describe ICU resource use in minor traumatic intracranial hemorrhage, we assess (1) the variability of ICU use in a cohort of patients with minor traumatic intracranial hemorrhage across multiple trauma centers, and (2) the proportion of adult patients with traumatic intracranial hemorrhage who are admitted to the ICU and never receive a critical care intervention during hospitalization. In addition, we evaluate the association between ICU admission and key independent variables.
Methods: A structured, historical cohort study of adult patients (aged 18 years and older) with minor traumatic intracranial hemorrhage was conducted within a consortium of 8 Level I trauma centers in the western United States from January 2005 to June 2010. The study population included patients with minor traumatic intracranial hemorrhage, defined as an emergency department (ED) Glasgow Coma Scale (GCS) score of 15 (normal mental status) and an Injury Severity Score less than 16 (no other major organ injury). The primary outcome measure was initial ICU admission. The secondary outcome measure was a critical care intervention during hospitalization. Critical care interventions included mechanical ventilation, neurosurgical intervention, transfusion of blood products, vasopressor or inotrope administration, and invasive hemodynamic monitoring. ED disposition and the proportion of ICU patients not receiving a critical care intervention were compared across sites with descriptive statistics. The association between ICU admission and predetermined independent variables was analyzed with multivariable regression.
Results: Among 11,240 adult patients with traumatic intracranial hemorrhage, 1,412 (13%) had minor traumatic intracranial hemorrhage and complete ED disposition data (mean age 48 years; SD 20 years). ICU use within this cohort across sites ranged from 50% to 97%. Overall, 847 of 888 patients (95%) with minor traumatic intracranial hemorrhage who were admitted to the ICU did not receive a critical care intervention during hospitalization (range between sites 80% to 100%). Three of 524 (0.6%) patients discharged home or admitted to the observation unit or ward received a critical care intervention. After controlling for severity of injury (age, blood pressure, and Injury Severity Score), study site was independently associated with ICU admission (odds ratios ranged from 1.5 to 30; overall effect P<.001).
Conclusion: Across a consortium of trauma centers in the western United States, there was wide variability in ICU use within a cohort of patients with minor traumatic intracranial hemorrhage. Moreover, a large proportion of patients admitted to the ICU never required a critical care intervention, indicating the potential to improve use of critical care resources in patients with minor traumatic intracranial hemorrhage.
Copyright © 2012 American College of Emergency Physicians. Published by Mosby, Inc. All rights reserved.
Figures

Comment in
-
Traumatic intracranial hemorrhage, value in health care, and being important.Ann Emerg Med. 2013 May;61(5):518-9. doi: 10.1016/j.annemergmed.2012.10.032. Epub 2012 Dec 20. Ann Emerg Med. 2013. PMID: 23261313 No abstract available.
References
-
- Ghajar J. Traumatic brain injury. Lancet. 2000;356:923–929. - PubMed
-
- Langlois JA, Rutland-Brown W, Thomas KE. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations, and Deaths. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Injury Prevention and Control; 2004.
-
- Vos PE, Battistin L, Birbamer G, et al. EFNS guideline on mild traumatic brain injury: report of an EFNS task force. Eur J Neurol. 2002;9:207–219. - PubMed
-
- Stiell IG, Clement CM, Rowe BH, et al. Comparison of the Canadian CT Head Rule and the New Orleans Criteria in patients with minor head injury. JAMA. 2005;294:1511–1518. - PubMed
-
- Wang MC, Linnau KF, Tirschwell DL, et al. Utility of repeat head computed tomography after blunt head trauma: a systematic review. J Trauma. 2006;61:226–233. - PubMed
Publication types
MeSH terms
Grants and funding
- L30 TR000286/TR/NCATS NIH HHS/United States
- UL1 RR025764/RR/NCRR NIH HHS/United States
- UL1 RR025780/RR/NCRR NIH HHS/United States
- 1UL1 RR025744/RR/NCRR NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- UL1 RR025014/RR/NCRR NIH HHS/United States
- UL1 TR001085/TR/NCATS NIH HHS/United States
- UL1 RR024146/RR/NCRR NIH HHS/United States
- C06 RR011234/RR/NCRR NIH HHS/United States
- UL1 RR025744/RR/NCRR NIH HHS/United States
- KL2 TR000421/TR/NCATS NIH HHS/United States
- UL1 RR024140/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
