

Obesity, systemic inflammation, and increased risk for cardiovascular disease and diabetes among adolescents: a need for screening tools to target interventions
- PMID: 23022122
- PMCID: PMC3578702
- DOI: 10.1016/j.nut.2012.07.003
Obesity, systemic inflammation, and increased risk for cardiovascular disease and diabetes among adolescents: a need for screening tools to target interventions
Abstract
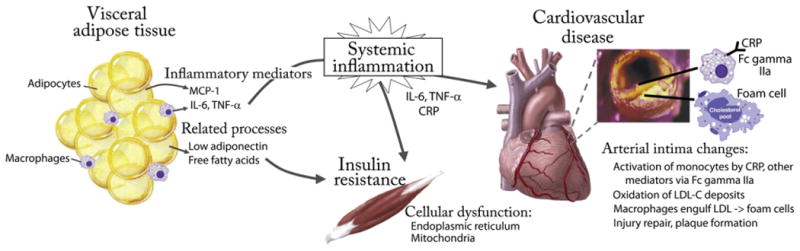
Cardiovascular disease (CVD) and type 2 diabetes mellitus have their roots in childhood, particularly in obese children and adolescents, raising important opportunities for early lifestyle intervention in at-risk individuals. However, not all obese individuals are at the same risk for disease progression. Accurate screening of obese adolescents may identify those in greatest need for intensive intervention to prevent or delay future disease. One potential screening target is obesity-related inflammation, which contributes to insulin resistance, metabolic syndrome, and CVD. In adults, the inflammatory marker high-sensitivity C-reactive protein (hsCRP) has utility for risk stratification and treatment initiation in individuals of intermediate CVD risk. In adolescents, hsCRP shares many of the associations of hsCRP in adults regarding the degree of insulin resistance, metabolic syndrome, and carotid artery media thickness. However, long-term data linking increased hsCRP levels-and increased insulin or decreased adiponectin-in childhood to adult disease outcomes are lacking at this time. Future efforts continue to be needed to identify childhood clinical and laboratory characteristics that could be used as screening tests to predict adult disease progression. Such tests may have utility in motivating physicians and patients' families toward lifestyle changes, ultimately improving prevention efforts.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
References
-
- Wilson PW, D'Agostino RB, Sullivan L, Parise H, Kannel WB. Overweight and obesity as determinants of cardiovascular risk: the Framingham experience. Arch Intern Med. 2002;162:1867–72. - PubMed
-
- Juonala M, Magnussen CG, Berenson GS, Venn A, Burns TL, Sabin MA, et al. Childhood adiposity, adult adiposity, and cardiovascular risk factors. N Engl J Med. 2011;365:1876–85. - PubMed
-
- Wildman RP, Muntner P, Reynolds K, McGinn AP, Rajpathak S, Wylie-Rosett J, et al. The obese without cardiometabolic risk factor clustering and the normal weight with cardiometabolic risk factor clustering: prevalence and correlates of 2 phenotypes among the US population (NHANES 1999–2004) Arch Intern Med. 2008;168:1617–24. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
