

Bone disease in primary hyperparathyrodism
- PMID: 23024712
- PMCID: PMC3458615
- DOI: 10.1177/1759720X12441869
Bone disease in primary hyperparathyrodism
Abstract
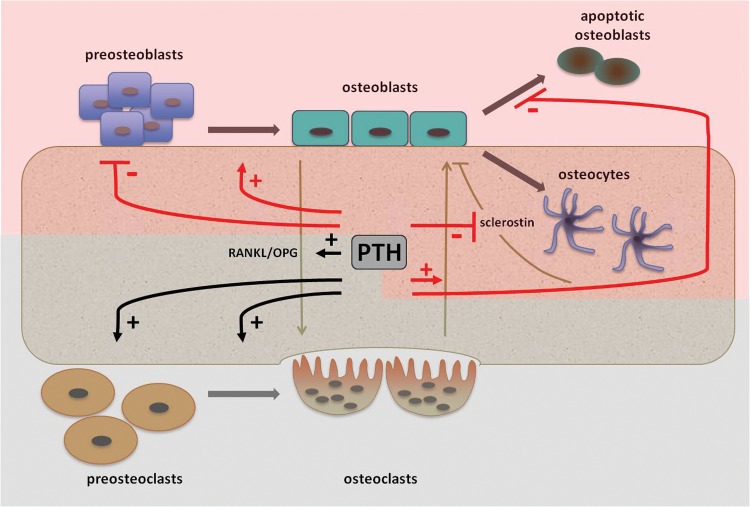
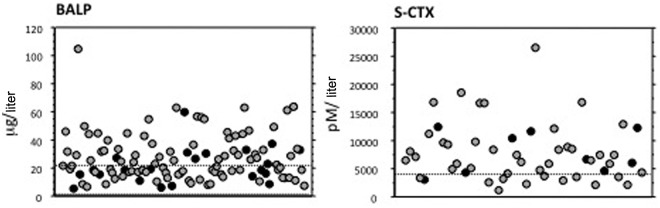
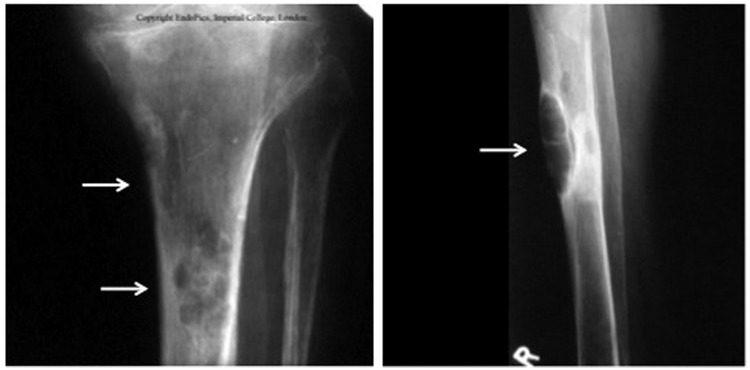
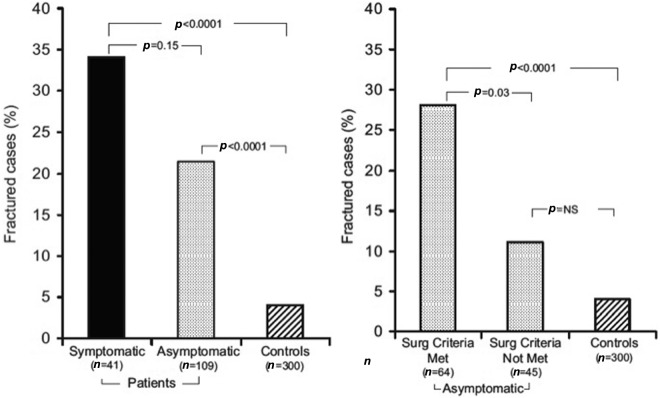
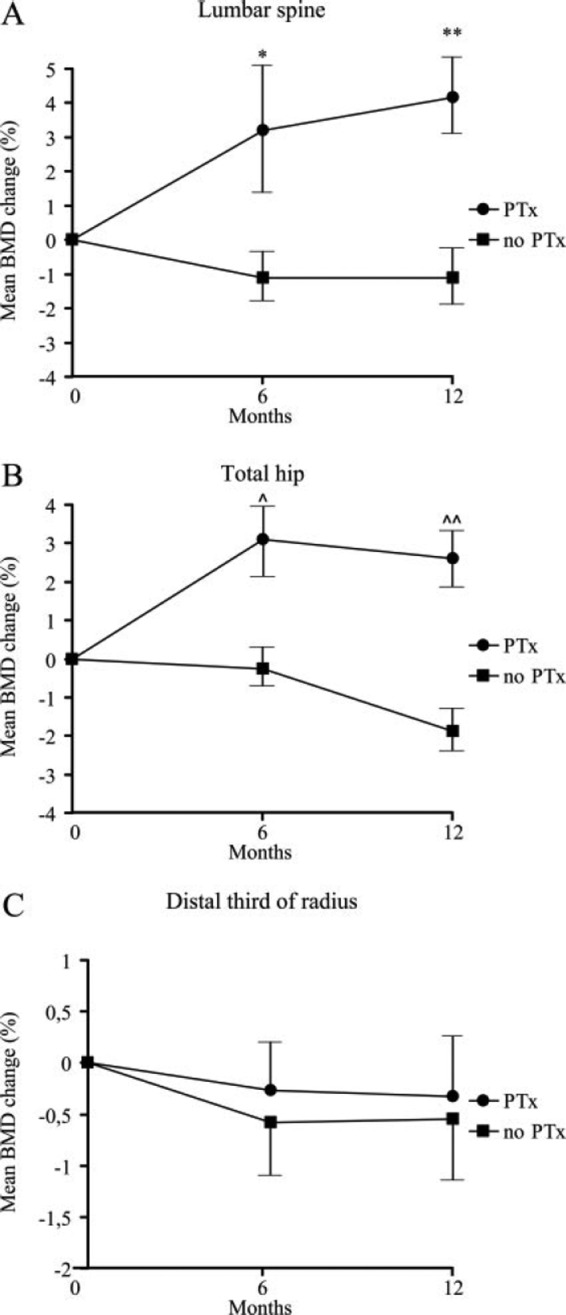
Nowadays, primary hyperparathyroidism (PHPT) is mostly a mild disease. Overt skeletal manifestations are rare but decreased bone mineral density (BMD) can still be demonstrated. Even in mild cases, excess parathyroid hormone (PTH) increases bone turnover leading to bone loss particularly at cortical sites. Conversely, a relative preservation of cancellous bone has been shown by histomorphometric analyses and advanced imaging techniques. An increased fracture rate has been demonstrated in untreated patients with PHPT at peripheral sites and in the spine. Parathyroidectomy (PTx) is the definitive cure for PHPT. With the restoration of normal PTH, bone resorption is quickly tapered down, while bone formation proceeds at the level of bone multicellular units, which were activated prior to PTx. The rapid refilling of the enlarged remodeling space and the subsequent matrix mineralization will result in an increase in BMD at sites rich in trabecular bone, such as lumbar spine and hip, which mainly occurs during the first 6-12 months after PTx. Cortical bone is less responsive to PTX because of the low rate of bone turnover, but sensible increases in BMD at the distal third of the radius can be observed in the long term. PTx seems to decrease the risk of fractures but more data are needed before a definitive conclusion on this important matter can be reached. Treatment with bisphosphonates can be considered for patients with low BMD who do not undergo PTx. Two-year treatment with alendronate has been shown to decrease bone turnover markers and increase BMD at the lumbar spine and hip, but not at the distal radius. Cinacalcet stably decreased serum calcium levels across a broad range of PHPT severity, but no change in BMD occurred in patients treated for up to 5.5 years.
Keywords: bisphosphonates; bone markers; bone mineral density; calcimimetics; histomorphometry; osteitis fibrosa cystica; parathyroid hormone; parathyroidectomy.
Figures
Similar articles
-
Marked and sustained increase in bone mineral density after parathyroidectomy in patients with primary hyperparathyroidism; a six-year longitudinal study with or without parathyroidectomy in a Japanese population.Clin Endocrinol (Oxf). 2004 Mar;60(3):335-42. doi: 10.1111/j.1365-2265.2004.01984.x. Clin Endocrinol (Oxf). 2004. PMID: 15008999
-
Primary hyperparathyroidism and the skeleton.Clin Endocrinol (Oxf). 2008 Jul;69(1):1-19. doi: 10.1111/j.1365-2265.2007.03162.x. Epub 2008 Jul 1. Clin Endocrinol (Oxf). 2008. PMID: 18167138 Review.
-
An Updated Perspective of the Clinical Features and Parathyroidectomy Impact in Primary Hyperparathyroidism Amid Multiple Endocrine Neoplasia Type 1 (MEN1): Focus on Bone Health.J Clin Med. 2025 Apr 30;14(9):3113. doi: 10.3390/jcm14093113. J Clin Med. 2025. PMID: 40364143 Free PMC article. Review.
-
Evaluation of changes in bone density and biochemical parameters after parathyroidectomy in primary hyperparathyroidism.Endocr J. 2000 Jun;47(3):231-7. doi: 10.1507/endocrj.47.231. Endocr J. 2000. PMID: 11036865 Clinical Trial.
-
Forestalling Hungry Bone Syndrome after Parathyroidectomy in Patients with Primary and Renal Hyperparathyroidism.Diagnostics (Basel). 2023 Jun 2;13(11):1953. doi: 10.3390/diagnostics13111953. Diagnostics (Basel). 2023. PMID: 37296804 Free PMC article. Review.
Cited by
-
Osseous Manifestations of Primary Hyperparathyroidism: Imaging Findings.Int J Endocrinol. 2020 Feb 21;2020:3146535. doi: 10.1155/2020/3146535. eCollection 2020. Int J Endocrinol. 2020. PMID: 32148487 Free PMC article. Review.
-
Osteolytic lesions: osteitis fibrosa cystica in the setting of severe primary hyperparathyroidism.BMJ Case Rep. 2017 May 28;2017:bcr2017220603. doi: 10.1136/bcr-2017-220603. BMJ Case Rep. 2017. PMID: 28554885 Free PMC article.
-
[Clinical polymorphism of primary hyperparathyroidism in children].Probl Endokrinol (Mosk). 2025 May 20;71(2):93-101. doi: 10.14341/probl13489. Probl Endokrinol (Mosk). 2025. PMID: 40411334 Free PMC article. Russian.
-
US-guided high-intensity focused ultrasound as a promising non-invasive method for treatment of primary hyperparathyroidism.Eur Radiol. 2014 Sep;24(9):2052-8. doi: 10.1007/s00330-014-3252-4. Epub 2014 Jun 4. Eur Radiol. 2014. PMID: 24895038
-
Clinical and Genetic Analysis of Multiple Endocrine Neoplasia Type 1-Related Primary Hyperparathyroidism in Chinese.PLoS One. 2016 Nov 15;11(11):e0166634. doi: 10.1371/journal.pone.0166634. eCollection 2016. PLoS One. 2016. PMID: 27846313 Free PMC article.
References
-
- Ambrogini E., Cetani F., Cianferotti L., Vignali E., Banti C., Viccica G., et al. (2007) Surgery or surveillance for mild asymptomatic primary hyperparathyroidism: a prospective, randomized clinical trial. J Clin Endocrinol Metab 92: 3114–3121 - PubMed
-
- Bellido T., Ali A.A., Plotkin L.I., Fu Q., Gubrij I., Roberson P.K., et al. (2003) Proteasomal degradation of Runx2 shortens parathyroid hormone-induced anti-apoptotic signaling in osteoblasts. A putative explanation for why intermittent administration is needed for bone anabolism. J Biol Chem 278: 50259–50272 - PubMed
-
- Bilezikian J.P., Silverberg S.J. (2000) Clinical spectrum of primary hyperparathyrodiism. Rev Endoc Metab Disord 1: 237–245 - PubMed
-
- Bilezikian J.P., Khan A.A., Potts J.T., Jr on behalf of the Third International Workshop on the Management of Asymptomatic Primary Hyperthyroidism (2009) Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the Third International Workshop. J Clin Endocrinol Metab 94: 335–339 - PMC - PubMed
-
- Bilezikian J.P., Potts J.T., Jr, Fuleihan Gel-H., Kleerekoper M., Neer R., Peacock M., et al. (2002) Summary statement from a workshop on asymptomatic primary hyperparathyroidism. A perspective for the 21st century. J Clin Endocrinol Metab 87: 5353–5361 - PubMed
LinkOut - more resources
Full Text Sources
