

Thyrotropin-blocking autoantibodies and thyroid-stimulating autoantibodies: potential mechanisms involved in the pendulum swinging from hypothyroidism to hyperthyroidism or vice versa
- PMID: 23025526
- PMCID: PMC3539254
- DOI: 10.1089/thy.2012.0374
Thyrotropin-blocking autoantibodies and thyroid-stimulating autoantibodies: potential mechanisms involved in the pendulum swinging from hypothyroidism to hyperthyroidism or vice versa
Abstract
Background: Thyrotropin receptor (TSHR) antibodies that stimulate the thyroid (TSAb) cause Graves' hyperthyroidism and TSHR antibodies which block thyrotropin action (TBAb) are occasionally responsible for hypothyroidism. Unusual patients switch from TSAb to TBAb (or vice versa) with concomitant thyroid function changes. We have examined case reports to obtain insight into the basis for "switching."
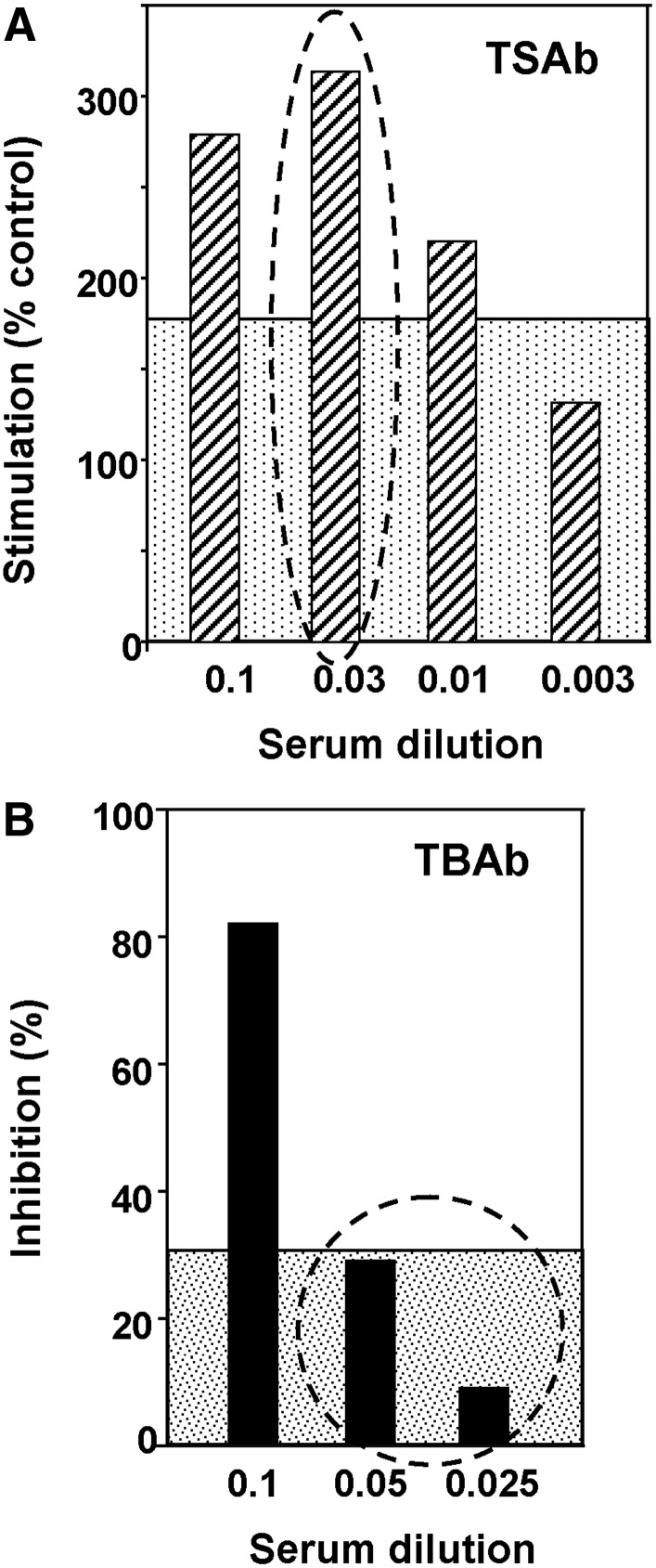
Summary: TBAb to TSAb switching occurs in patients treated with levothyroxine (LT4); the reverse switch (TBAb to TSAb) occurs after anti-thyroid drug therapy; TSAb/TBAb alterations may occur during pregnancy and are well recognized in transient neonatal thyroid dysfunction. Factors that may impact the shift include: (i) LT4 treatment, usually associated with decreased thyroid autoantibodies, in unusual patients induces or enhances thyroid autoantibody levels; (ii) antithyroid drug treatment decreases thyroid autoantibody levels; (iii) hyperthyroidism can polarize antigen-presenting cells, leading to impaired development of regulatory T cells, thereby compromising control of autoimmunity; (iv) immune-suppression/hemodilution reduces thyroid autoantibodies during pregnancy and rebounds postpartum; (v) maternally transferred IgG transiently impacts thyroid function in neonates until metabolized; (vi) a Graves' disease model involving immunizing TSHR-knockout mice with mouse TSHR-adenovirus and transfer of TSHR antibody-secreting splenocytes to athymic mice demonstrates the TSAb to TBAb shift, paralleling the outcome of maternally transferred "term limited" TSHR antibodies in neonates. Finally, perhaps most important, as illustrated by dilution analyses of patients' sera in vitro, TSHR antibody concentrations and affinities play a critical role in switching TSAb and TBAb functional activities in vivo.
Conclusions: Switching between TBAb and TSAb (or vice versa) occurs in unusual patients after LT4 therapy for hypothyroidism or anti-thyroid drug treatment for Graves' disease. These changes involve differences in TSAb versus TBAb concentrations, affinities and/or potencies in individual patients. Thus, anti-thyroid drugs or suppression/hemodilution in pregnancy reduce initially low TSAb levels even further, leading to TBAb dominance. In contrast, TSAb emergence after LT4 administration may be sufficient to counteract TBAb inhibition. The occurrence of "switching" emphasizes the need for careful patient monitoring and management. Finally, whole genome screening of relatively rare "switch" patients and appropriate Graves' and Hashimoto's controls could provide unexpected and valuable information regarding the basis for thyroid autoimmunity.
Figures
References
-
- Rapoport B. Chazenbalk GD. Jaume JC. McLachlan SM. The thyrotropin receptor: interaction with thyrotropin and autoantibodies. Endocr Rev. 1998;19:673–716. - PubMed
-
- Orgiazzi J. Williams DE. Chopra IJ. Solomon DH. Human thyroid adenyl cyclase-stimulating activity in immunoglobulin G of patients with Graves' disease. J Clin Endocrinol Metab. 1976;42:341–354. - PubMed
-
- Endo K. Kasagi K. Konishi J. Ikekubo K. Tatsuyo O. Takeda Y. Mori T. Torizuka K. Detection and properties of TSH-binding inhibitor immunoglobulins in patients with Graves' disease and Hashimoto's thyroiditis. J Clin Endocrinol Metab. 1978;46:734–739. - PubMed
-
- Matsuura N. Yamada Y. Nohara Y. Konishi J. Kasagi K. Endo K. Kojima K. Wataya K. Familial neonatal transient hypothyroidism due to maternal TSH-binding inhibitor immunoglobulins. N Engl J Med. 1980;303:738–741. - PubMed
-
- Evans M. Sanders J. Tagami T. Sanders P. Young S. Roberts E. Wilmot J. Hu X. Kabelis K. Clark J. Holl S. Richards T. Collyer A. Furmaniak J. Smith BR. Monoclonal autoantibodies to the TSH receptor, one with stimulating activity and one with blocking activity, obtained from the same blood sample. Clin Endocrinol (Oxf) 2010;73:404–412. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
