

Prediction of Contrast-Induced Nephropathy With Persistent Renal Dysfunction and Adverse Long-term Outcomes in Patients With Acute Myocardial Infarction Using the Mehran Risk Score
- PMID: 23027701
- PMCID: PMC6649613
- DOI: 10.1002/clc.22060
Prediction of Contrast-Induced Nephropathy With Persistent Renal Dysfunction and Adverse Long-term Outcomes in Patients With Acute Myocardial Infarction Using the Mehran Risk Score
Abstract
Background: Contrast-induced nephropathy (CIN) has been generally considered to be transient and associated with unfavorable clinical outcomes.
Hypothesis: The aim of this study was to investigate whether Mehran risk score could predict CIN with persistent renal dysfunction and long-term clinical outcomes in acute myocardial infarction (AMI) patients undergoing percutaneous coronary intervention (PCI).
Methods: We analyzed the clinical data of 1041 AMI patients. The primary end point was defined as major adverse cardiovascular and cerebrovascular event (MACCE) including death, reinfarction, target vessel revascularization, heart failure requiring hospital admission, and stroke. Patients were categorized into 4 groups according to risk scores: low (≤ 5, n = 596), moderate (6-10, n = 265), high (11-15, n = 111), and very high (≥16, n = 69).
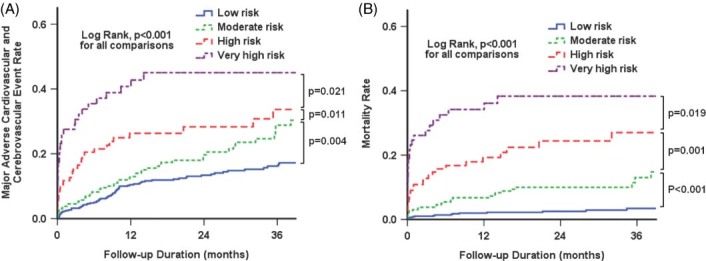
Results: Among the 148 patients (14.2%) who developed CIN, persistent renal dysfunction was observed in 68 patients. Presence in high- or very high-risk groups was the most important independent risk factor of CIN with persistent renal dysfunction (odds ratio: 3.35, 95 confidence interval [CI]: 1.89-5.92, P < 0.001). Furthermore, patients in higher-risk groups experienced significantly more MACCE and mortality 2 years after PCI. Using multivariate analysis, significant increase in the hazard ratio (HR) for MACCE was noted in moderate- (HR: 1.40, 95% CI: 0.97-2.03, P = 0.075), high- (HR 1.96, 95% CI: 1.22-3.15, P = 0.006), and very high-risk (HR 2.40, 95% CI: 1.36-4.21, p = 0.002) groups, compared with the low-risk group. The very high-risk group had approximately 6-fold increase in mortality over the low-risk group (HR: 6.22, 95% CI: 2.77-13.95, P < 0.001).
Conclusions: Mehran risk score predicted CIN with persistent renal dysfunction and long-term clinical outcomes in patients with AMI.
© 2012 Wiley Periodicals, Inc.
Figures
References
-
- McCullough PA, Adam A, Becker CR, et al. Epidemiology and prognostic implications of contrast‐induced nephropathy. Am J Cardiol. 2006;98:5K–13K. - PubMed
-
- Best PJ, Lennon R, Ting HH, et al. The impact of renal insufficiency on clinical outcomes in patients undergoing percutaneous coronary interventions. J Am Coll Cardiol. 2002;39: 1113–1119. - PubMed
-
- Parfrey PS, Griffiths SM, Barrett BJ, et al. Contrast material‐induced renal failure in patients with diabetes mellitus, renal insufficiency, or both. A prospective controlled study. N Engl J Med. 1989;320:143–149. - PubMed
-
- Rihal CS, Textor SC, Grill DE, et al. Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation. 2002;105:2259–2264. - PubMed
-
- Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score for prediction of contrast‐induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. 2004;44:1393–1399. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
