

Mechanisms of human atrial fibrillation initiation: clinical and computational studies of repolarization restitution and activation latency
- PMID: 23027797
- PMCID: PMC3833353
- DOI: 10.1161/CIRCEP.111.969022
Mechanisms of human atrial fibrillation initiation: clinical and computational studies of repolarization restitution and activation latency
Abstract
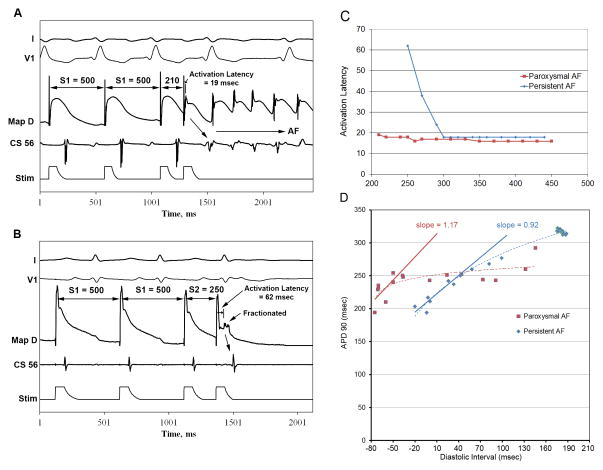
Background: Mechanisms of atrial fibrillation (AF) initiation are incompletely understood. We hypothesized that rate-dependent changes (restitution) in action potential duration (APD) and activation latency are central targets for clinical interventions that induce AF. We tested this hypothesis using clinical experiments and computer models.
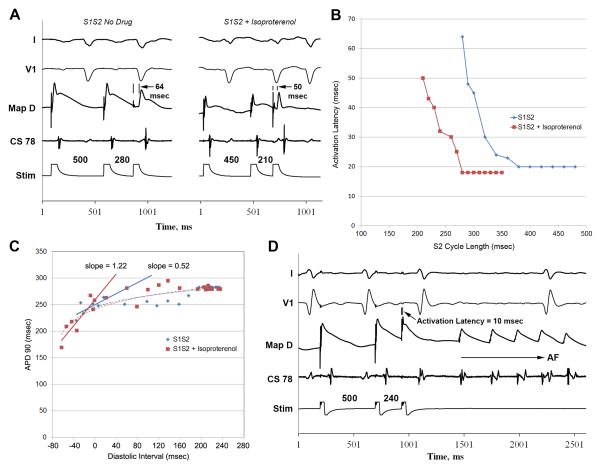
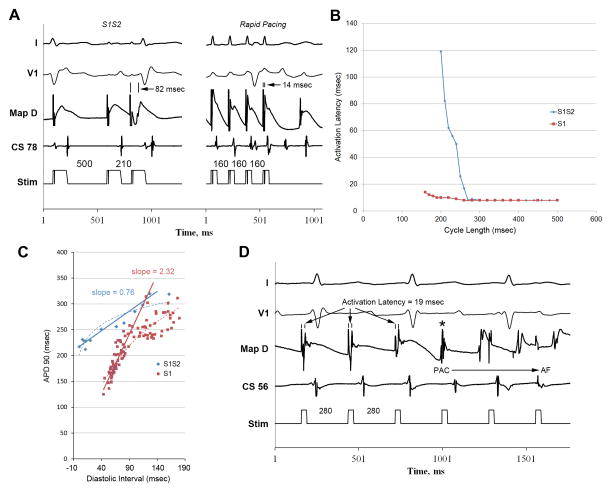
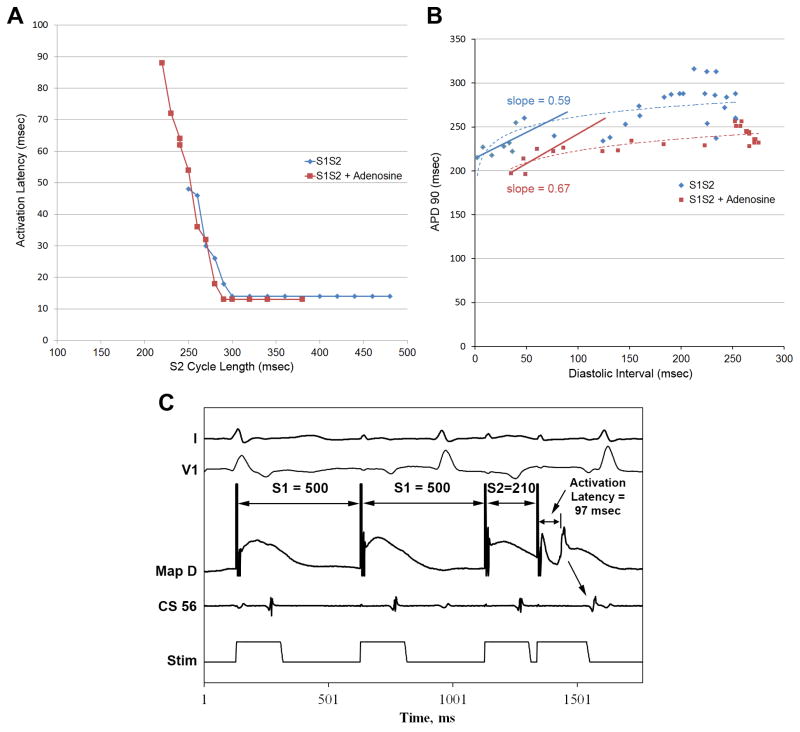
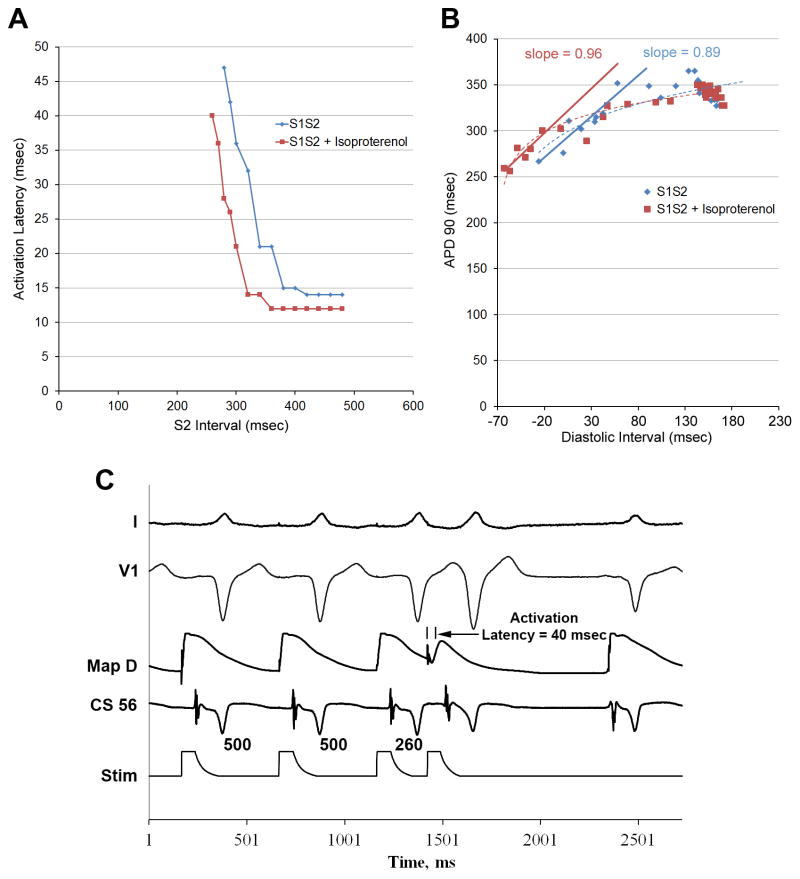
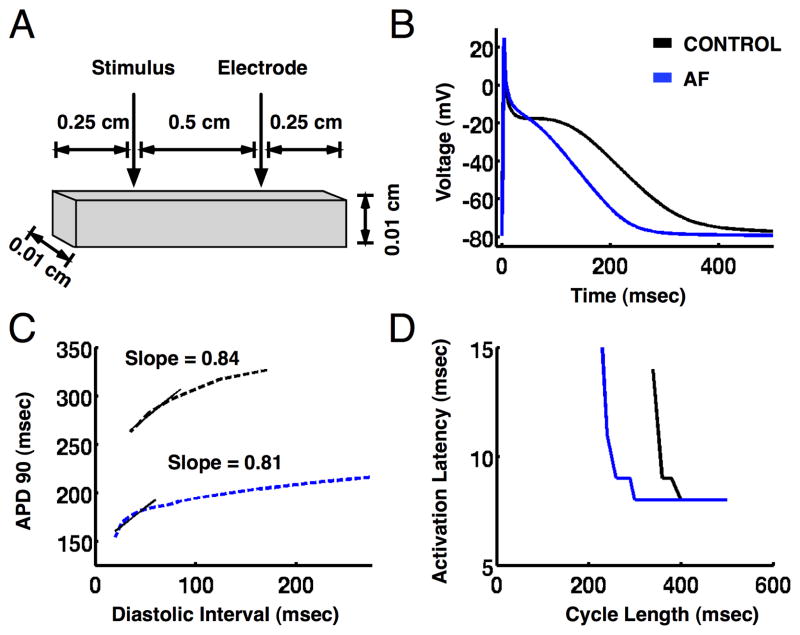
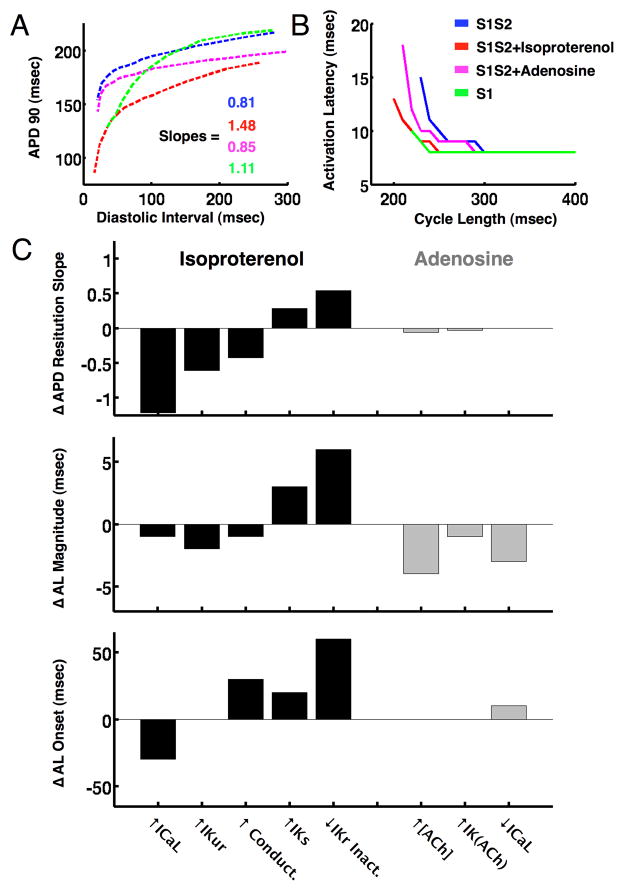
Methods and results: In 50 patients (20 persistent, 23 paroxysmal AF, 7 controls), we used monophasic action potential catheters to define left atrial APD restitution, activation latency, and AF incidence from premature extrastimuli. Isoproterenol (n=14), adenosine (n=10), or rapid pacing (n=36) was then initiated to determine impact on these parameters. Compared with baseline in AF patients, isoproterenol and rapid pacing decreased activation latency (64±14 versus 31±13 versus 24±14 ms; P<0.05), steepened maximum APD restitution slope (0.8±0.7 versus 1.7±0.5 versus 1.1±0.5; P<0.05), and increased AF incidence (12% versus 64% versus 84%; P<0.05). Conversely, adenosine shortened APD (P<0.05), yet increased activation latency (86±27 ms; P=0.002) so that maximum APD restitution slope did not steepen (1.0±0.5; P=NS), and AF incidence was unchanged (10%; P=NS). In controls, no intervention steepened APD restitution or initiated AF. Computational modeling revealed that isoproterenol steepened APD restitution by increased L-type calcium current and decreased activation latency via enhanced rapid delayed potassium reactifier current inactivation, whereas rapid pacing steepened APD restitution via increased cardiac inward potassium rectifier current.
Conclusions: Steep APD restitution is a common pathway for AF initiation by isoproterenol and tachycardia via reduced activation latency that enables engagement of steep APD restitution at rapid rates. Modeling suggests that AF initiation from each intervention uses distinct ionic mechanisms. This insight may help design interventions to prevent AF.
Conflict of interest statement
Figures
References
-
- Oakes RS, Badger TJ, Kholmovski EG, Akoum N, Burgon NS, Fish EN, Blauer JJ, Rao SN, DiBella EV, Segerson NM, Daccarett M, Windfelder J, McGann CJ, Parker D, MacLeod RS, Marrouche NF. Detection and quantification of left atrial structural remodeling with delayed-enhancement magnetic resonance imaging in patients with atrial fibrillation. Circulation. 2009;119:1758–1767. - PMC - PubMed
-
- Cherry EM, Ehrlich JR, Nattel S, Fenton FH. Pulmonary vein reentry--properties and size matter: Insights from a computational analysis. Heart rhythm. 2007;4:1553–1562. - PubMed
-
- Weiss JN, Karma A, Shiferaw Y, Chen PS, Garfinkel A, Qu Z. From pulsus to pulseless: The saga of cardiac alternans. Circ Res. 2006;98:1244–1253. - PubMed
-
- Rensma PL, Allessie MA, Lammers WJ, Bonke FI, Schalij MJ. Length of excitation wave and susceptibility to reentrant atrial arrhythmias in normal conscious dogs. Circ Res. 1988;62:395–410. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
