

Skeletal muscle vasodilatation during maximal exercise in health and disease
- PMID: 23027820
- PMCID: PMC3533191
- DOI: 10.1113/jphysiol.2012.241190
Skeletal muscle vasodilatation during maximal exercise in health and disease
Abstract
Maximal exercise vasodilatation results from the balance between vasoconstricting and vasodilating signals combined with the vascular reactivity to these signals. During maximal exercise with a small muscle mass the skeletal muscle vascular bed is fully vasodilated. During maximal whole body exercise, however, vasodilatation is restrained by the sympathetic system. This is necessary to avoid hypotension since the maximal vascular conductance of the musculature exceeds the maximal pumping capacity of the heart. Endurance training and high-intensity intermittent knee extension training increase the capacity for maximal exercise vasodilatation by 20-30%, mainly due to an enhanced vasodilatory capacity, as maximal exercise perfusion pressure changes little with training. The increase in maximal exercise vascular conductance is to a large extent explained by skeletal muscle hypertrophy and vascular remodelling. The vasodilatory capacity during maximal exercise is reduced or blunted with ageing, as well as in chronic heart failure patients and chronically hypoxic humans; reduced vasodilatory responsiveness and increased sympathetic activity (and probably, altered sympatholysis) are potential mechanisms accounting for this effect. Pharmacological counteraction of the sympathetic restraint may result in lower perfusion pressure and reduced oxygen extraction by the exercising muscles. However, at the same time fast inhibition of the chemoreflex in maximally exercising humans may result in increased vasodilatation, further confirming a restraining role of the sympathetic nervous system on exercise-induced vasodilatation. This is likely to be critical for the maintenance of blood pressure in exercising patients with a limited heart pump capacity.
Figures
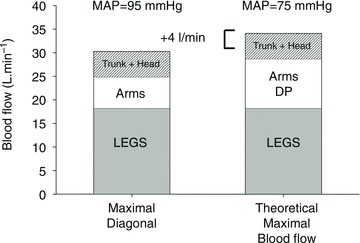
 ) skiing while using arm and legs (diagonal technique), only arm (double poling technique) and leg skiing (like skating). They were also studied during maximal exercise with the diagonal technique. Trunk and head perfusion at maximal diagonal was calculated by subtracting peak leg and arm blood flows from peak cardiac output. The maximal theoretical cardiac output was calculated by adding the maximal values that were observed for leg blood flow (during maximal diagonal), the peak arm blood flow (observed during double poling) and the 5 l min−1 of blood flow necessary to perfuse the head and trunk. The latter gave 4 l min1 more cardiac output than actually measured, implying that in humans with well trained arm and leg muscles the combined peak perfusion of the head trunk and arm muscle exceeds the pumping capacity of the heart. This also implies that during maximal upright arm and leg combined exercise, muscle vasodilatation must be restrained to avoid hypotension. (Figure from Calbet & Joyner, 2010.)
) skiing while using arm and legs (diagonal technique), only arm (double poling technique) and leg skiing (like skating). They were also studied during maximal exercise with the diagonal technique. Trunk and head perfusion at maximal diagonal was calculated by subtracting peak leg and arm blood flows from peak cardiac output. The maximal theoretical cardiac output was calculated by adding the maximal values that were observed for leg blood flow (during maximal diagonal), the peak arm blood flow (observed during double poling) and the 5 l min−1 of blood flow necessary to perfuse the head and trunk. The latter gave 4 l min1 more cardiac output than actually measured, implying that in humans with well trained arm and leg muscles the combined peak perfusion of the head trunk and arm muscle exceeds the pumping capacity of the heart. This also implies that during maximal upright arm and leg combined exercise, muscle vasodilatation must be restrained to avoid hypotension. (Figure from Calbet & Joyner, 2010.)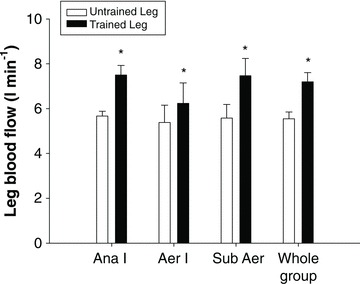
 by 32%, and this improvement was due to a 30% increase in leg blood flow (Whole group) (Blomstrand et al. 2011).
by 32%, and this improvement was due to a 30% increase in leg blood flow (Whole group) (Blomstrand et al. 2011).
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical