

The alternative complement pathway propagates inflammation and injury in murine ischemic stroke
- PMID: 23028050
- PMCID: PMC3478485
- DOI: 10.4049/jimmunol.1201904
The alternative complement pathway propagates inflammation and injury in murine ischemic stroke
Abstract
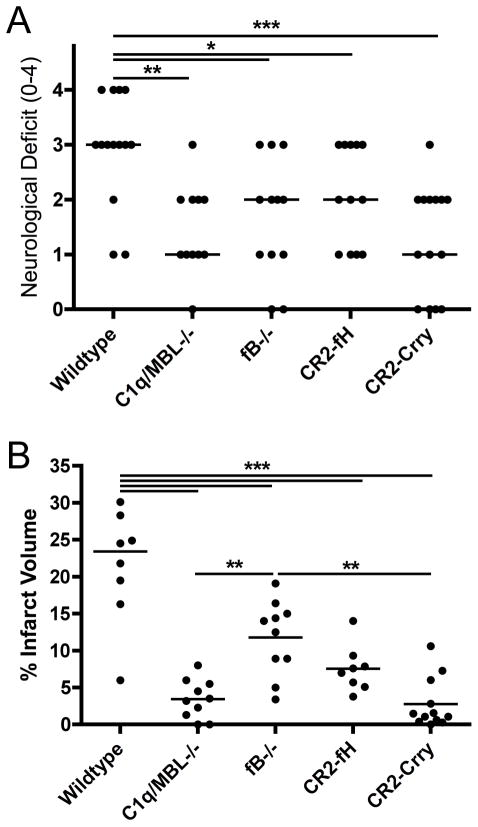
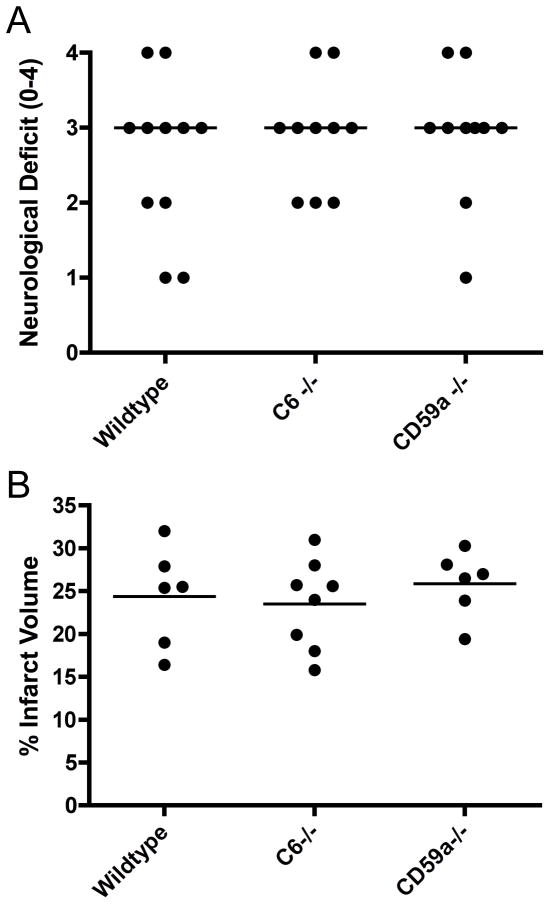
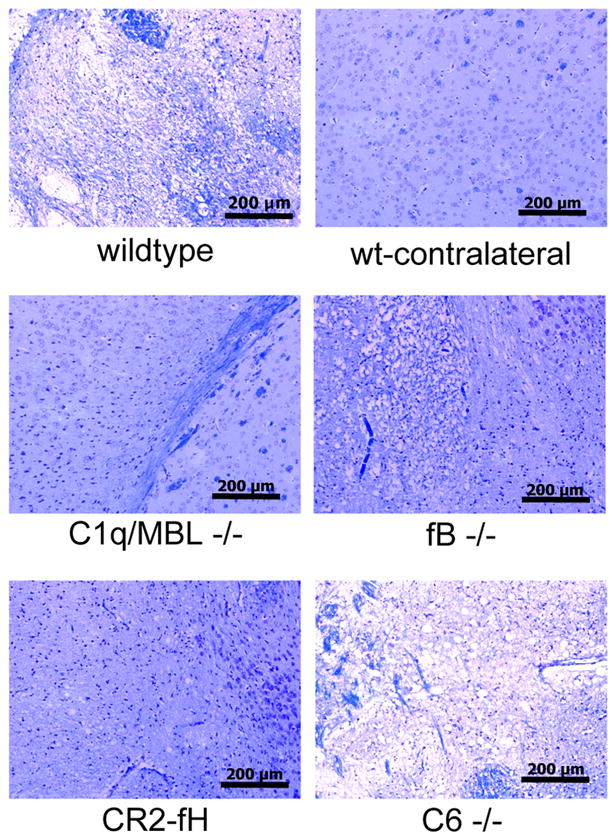
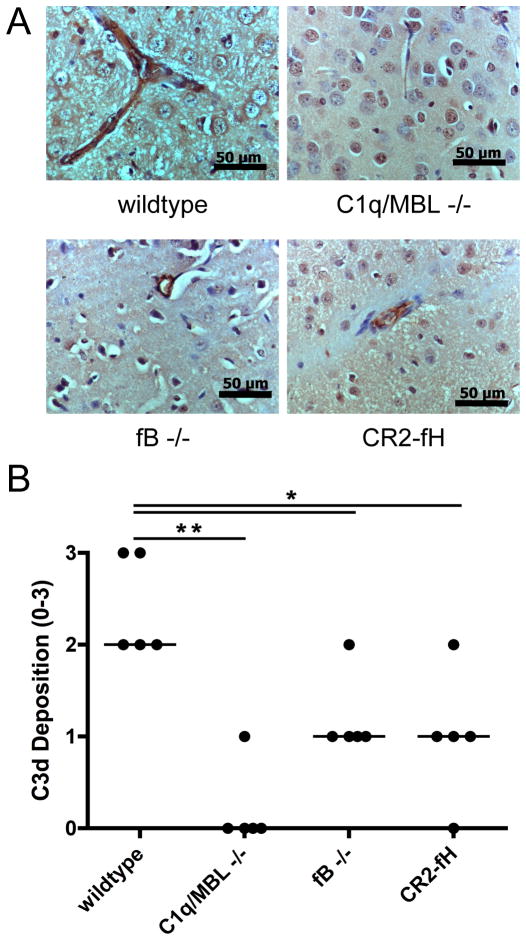
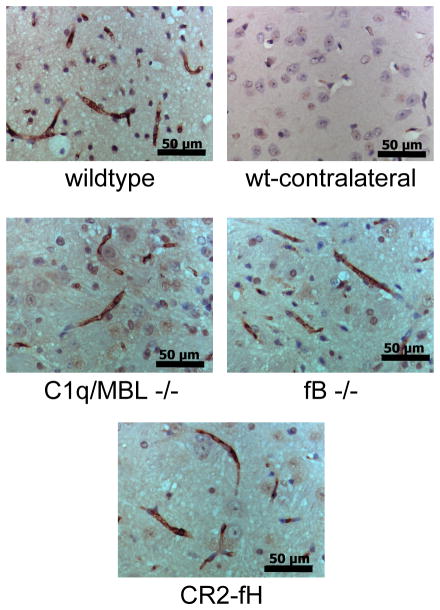
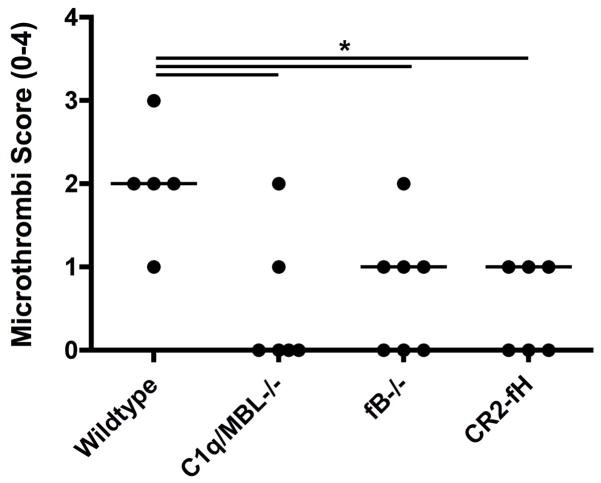
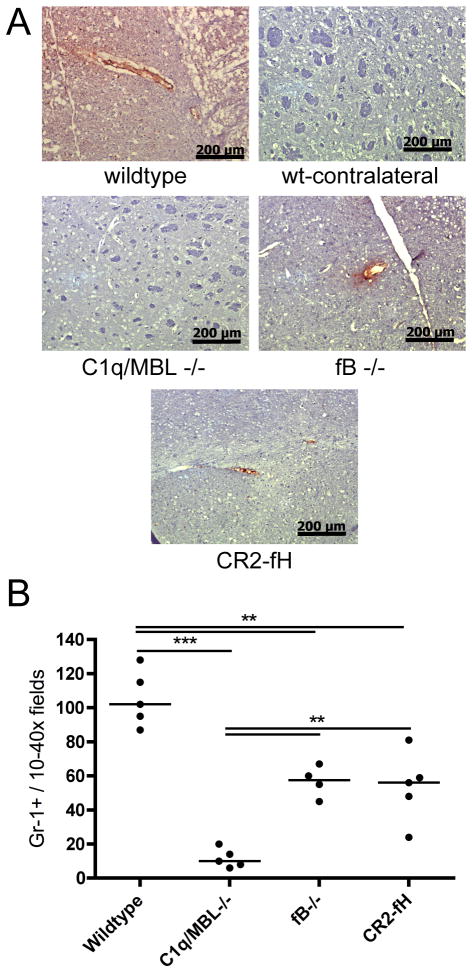
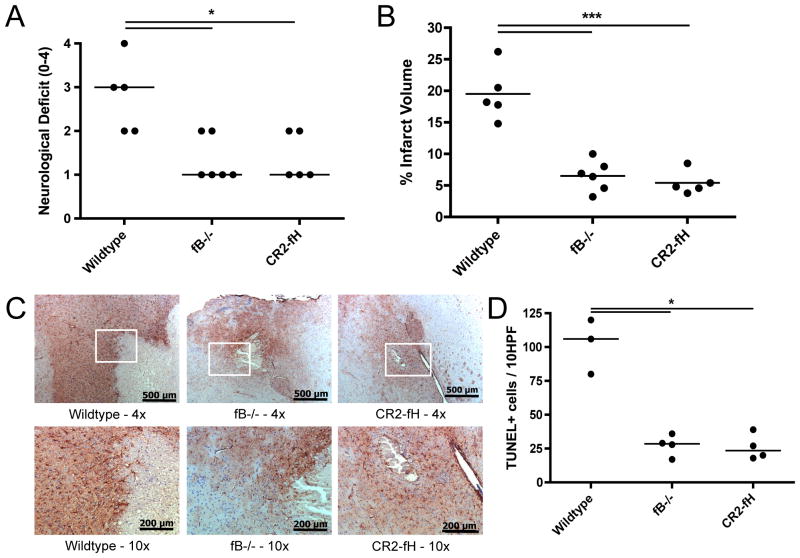
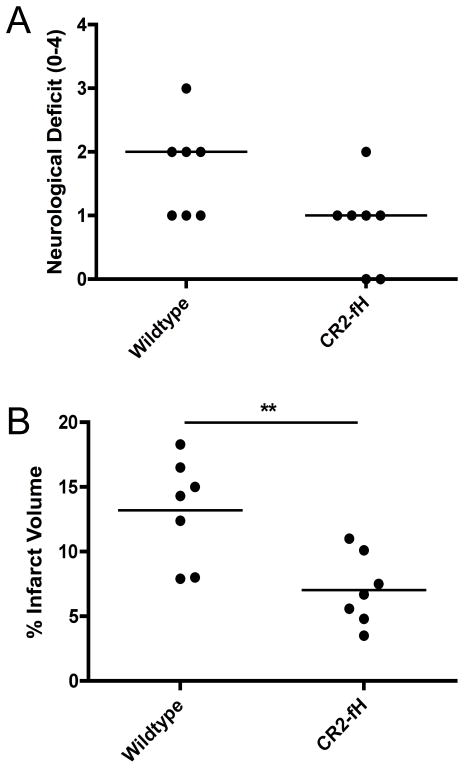
There is mounting evidence indicating an important role for complement in the pathogenesis of cerebral ischemia-reperfusion injury, or ischemic stroke. The role of the alternative complement pathway in ischemic stroke has not been investigated, and there is conflicting data on the role of the terminal pathway. In this study, we show that compared with wild-type mice, mice deficient in the alternative pathway protein factor B or mice treated with the alternative pathway inhibitor CR2-fH have improved outcomes after 60-min middle cerebral artery occlusion and 24-h reperfusion. Factor B-deficient or CR2-fH-treated mice were protected in terms of improved neurologic function and reduced cerebral infarct, demyelination, P-selectin expression, neutrophil infiltration, and microthrombi formation. Mice deficient in both the classical and lectin pathways (C1q/MBL deficient) were also protected from cerebral ischemia-reperfusion injury, and there was no detectable C3d deposition in the ipsilateral brain of these mice. These data demonstrate that the alternative pathway is not alone sufficient to initiate complement activation and indicate that the alternative pathway propagates cerebral injury via amplification of the cascade. Deficiency of C6, a component of the terminal cytolytic membrane attack complex, had no effect on outcome after ischemic stroke, indicating that the membrane attack complex is not involved in mediating injury in this model. We additionally show that the protective effect of factor B deficiency and CR2-fH treatment is sustained in the subacute stage of infarct development, adding to the clinical relevance of these findings.
Figures
References
-
- Dirnagl U, Iadecola C, Moskowitz MA. Pathobiology of ischaemic stroke: an integrated view. Trends Neurosci. 1999;22:391–397. - PubMed
-
- Schaller B, Graf R. Cerebral ischemia and reperfusion: the pathophysiologic concept as a basis for clinical therapy. J Cereb Blood Flow Metab. 2004;24:351–371. - PubMed
-
- Huang J, Kim LJ, Mealey R, Marsh HC, Jr, Zhang Y, Tenner AJ, Connolly ES, Jr, Pinsky DJ. Neuronal protection in stroke by an sLex-glycosylated complement inhibitory protein. Science. 1999;285:595–599. - PubMed
-
- Atkinson C, Zhu H, Qiao F, Varela JC, Yu J, Song H, Kindy MS, Tomlinson S. Complement-dependent P-selectin expression and injury following ischemic stroke. J Immunol. 2006;177:7266–7274. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
