

Reduced survival and quality of life following return to dialysis after transplant failure: the Dialysis Outcomes and Practice Patterns Study
- PMID: 23028105
- PMCID: PMC3616760
- DOI: 10.1093/ndt/gfs386
Reduced survival and quality of life following return to dialysis after transplant failure: the Dialysis Outcomes and Practice Patterns Study
Abstract
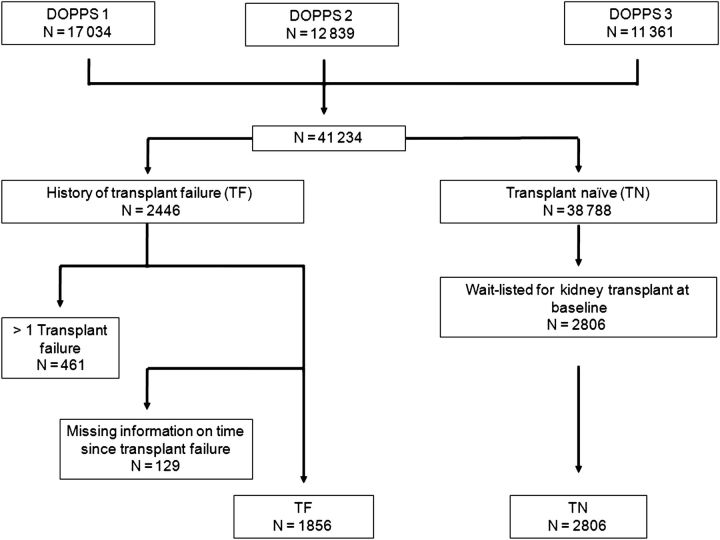
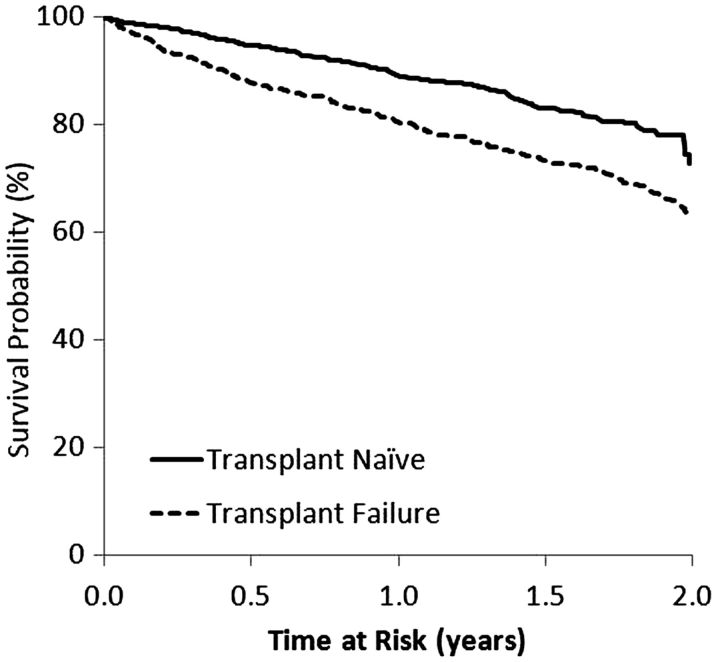
Background: Although dialysis after kidney transplant failure (TF) is common, the outcomes of these patients remain unclear. We compared outcomes of TF patients with transplant-naïve (TN) patients wait-listed for kidney transplantation.
Methods: We used data from the Dialysis Outcomes and Practice Patterns Study (DOPPS), including laboratory markers and health-related quality of life (HR-QOL). Mortality and hospitalization of participants with one prior TF versus TN patients were compared using the Cox regression analysis. HR-QOL physical and mental component summary scores (PCS and MCS) were examined using linear mixed models, and clinical practices were compared using logistic regression.
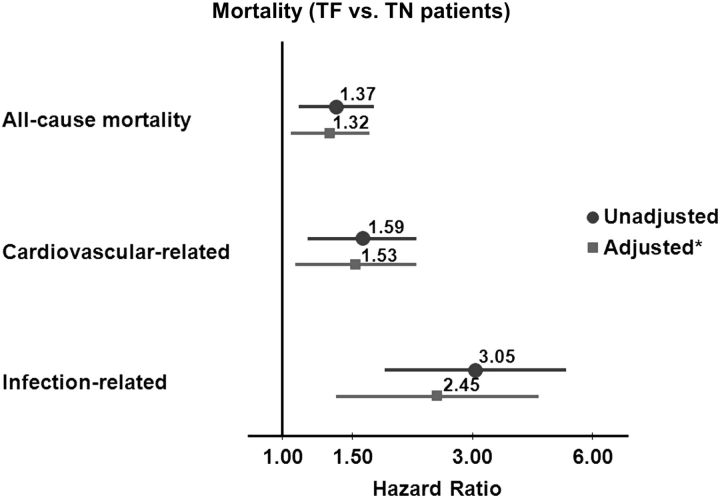
Results: Compared with TN patients (n = 2806), TF patients (n = 1856) were younger (48 versus 51 years, P = 0.003), less likely to be diabetic (18 versus 27%, P < 0.0001) and to use a permanent surgical vascular access {adjusted odds ratio (AOR): 0.85 [95% confidence interval (CI): 0.70-1.03], P = 0.10}, particularly within the first 3 months after TF [AOR 0.45 (0.32-0.62), P < 0.0001]. TF patients also had lower PCS [mean difference -2.56 (-3.36, -1.75), P < 0.0001] but not MCS [-0.42 (-1.34, 0.50), P = 0.37]. All-cause mortality [adjusted hazard ratio (AHR): 1.32 (95% CI: 1.05-1.66), P = 0.02], especially infection-related [AHR 2.45 (95% CI: 1.36-4.41), P = 0.01], was higher among TF patients.
Conclusions: TF patients have reduced QOL and higher mortality, particularly due to infections, than TN patients. Interventions to optimize care before and after starting dialysis remain to be identified and applied in clinical practice.
Figures
References
-
- Wolfe RA, Ashby VB, Milford EL, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341:1725–1730. doi:10.1056/NEJM199912023412303. - DOI - PubMed
-
- Laupacis A, Keown P, Pus N, et al. A study of the quality of life and cost-utility of renal transplantation. Kidney Int. 1996;50:235–242. doi:10.1038/ki.1996.307. - DOI - PubMed
-
- Lamb KE, Lodhi S, Meier-Kriesche HU. Long-term renal allograft survival in the United States: a critical reappraisal. Am J Transplant. 2011;11:450–462. doi:10.1111/j.1600-6143.2010.03283.x. - DOI - PubMed
-
- US Renal Data System: USRDS 2007 Annual Data Report. Bethesda: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2007.
-
- Gill JS, Abichandani R, Kausz AT, et al. Mortality after kidney transplant failure: the impact of non-immunologic factors. Kidney Int. 2002;62:1875–1883. doi:10.1046/j.1523-1755.2002.00640.x. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
