

Different patterns of cytokines and chemokines combined with IFN-γ production reflect Mycobacterium tuberculosis infection and disease
- PMID: 23028695
- PMCID: PMC3441719
- DOI: 10.1371/journal.pone.0044944
Different patterns of cytokines and chemokines combined with IFN-γ production reflect Mycobacterium tuberculosis infection and disease
Abstract
Background: IFN-γ is presently the only soluble immunological marker used to help diagnose latent Mycobacterium tuberculosis (M.tb) infection. However, IFN-γ is not available to distinguish latent from active TB infection. Moreover, extrapulmonary tuberculosis, such as tuberculous pleurisy, cannot be properly diagnosed by IFN-γ release assay. As a result, other disease- or infection-related immunological biomarkers that would be more effective need to be screened and identified.
Methodology: A panel of 41 soluble immunological molecules (17 cytokines and 24 chemokines) was tested using Luminex liquid array-based multiplexed immunoassays. Samples, including plasma and pleural effusions, from healthy donors (HD, n = 12) or patients with latent tuberculosis infection (LTBI, n = 20), pulmonary tuberculosis (TB, n = 12), tuberculous pleurisy (TP, n = 15) or lung cancer (LC, n = 15) were collected and screened for soluble markers. Peripheral blood mononuclear cells (PBMCs) and pleural fluid mononuclear cells (PFMCs) were also isolated to investigate antigen-specific immune factors.
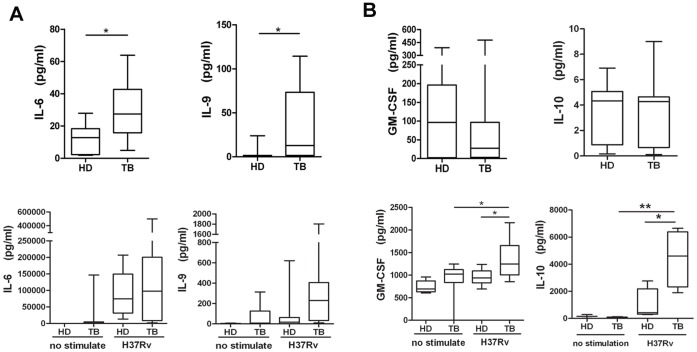
Principal findings: For the 41 examined factors, our results indicated that three patterns were closely associated with infection and disease. (1) Significantly elevated plasma levels of IL-2, IP-10, CXCL11 and CXCL12 were present in both patients with tuberculosis and in a sub-group participant with latent tuberculosis infection who showed a higher level of IFN-γ producing cells by ELISPOT assay compared with other latently infected individuals. (2) IL-6 and IL-9 were only significantly increased in plasma from active TB patients, and the two factors were consistently highly secreted after M.tb antigen stimulation. (3) When patients developed tuberculous pleurisy, CCL1, CCL21 and IL-6 were specifically increased in the pleural effusions. In particular, these three factors were consistently highly secreted by pleural fluid mononuclear cells following M.tb-specific antigen stimulation. In conclusion, our data imply that the specific secretion of soluble immunological factors, in addition to IFN-γ, may be used to evaluate M.tb infection and tuberculosis disease.
Conflict of interest statement
Figures



References
-
- WHO (2010) Report: Global tuberculosis control.
-
- WHO (2008) Report : Stop TB Partnership.
-
- Pathan AA, Wilkinson KA, Klenerman P, McShane H, Davidson RN, et al. (2001) Direct ex vivo analysis of antigen-specific IFN-gamma-secreting CD4 T cells in Mycobacterium tuberculosis-infected individuals: associations with clinical disease state and effect of treatment. J Immunol 167: 5217–5225. - PubMed
-
- Warier A, Gunawathi S, Venkatesh, John KR, Bose A (2010) T-cell assay as a diagnostic tool for tuberculosis. Indian Pediatr 47: 90–92. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
