

T-cell phenotypes, apoptosis and inflammation in HIV+ patients on virologically effective cART with early atherosclerosis
- PMID: 23029393
- PMCID: PMC3459872
- DOI: 10.1371/journal.pone.0046073
T-cell phenotypes, apoptosis and inflammation in HIV+ patients on virologically effective cART with early atherosclerosis
Abstract
Objective: We investigated the potential relationship between T-cell phenotype, inflammation, endotoxemia, and atherosclerosis evaluated by carotid intima-media thickness (IMT) in a cohort of HIV-positive patients undergoing long-term virologically suppressive combination antiretroviral therapy (cART).
Design: We studied 163 patients receiving virologically suppressive cART.
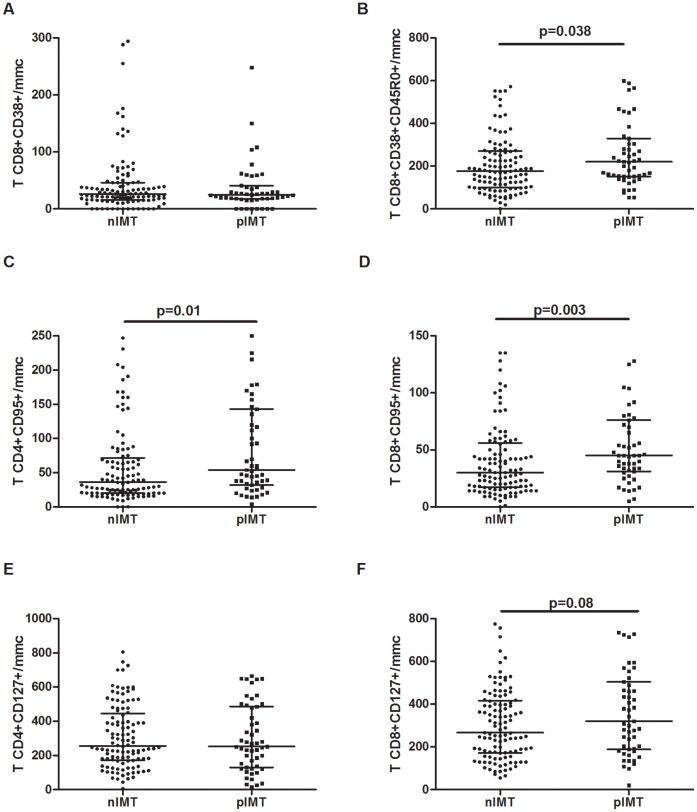
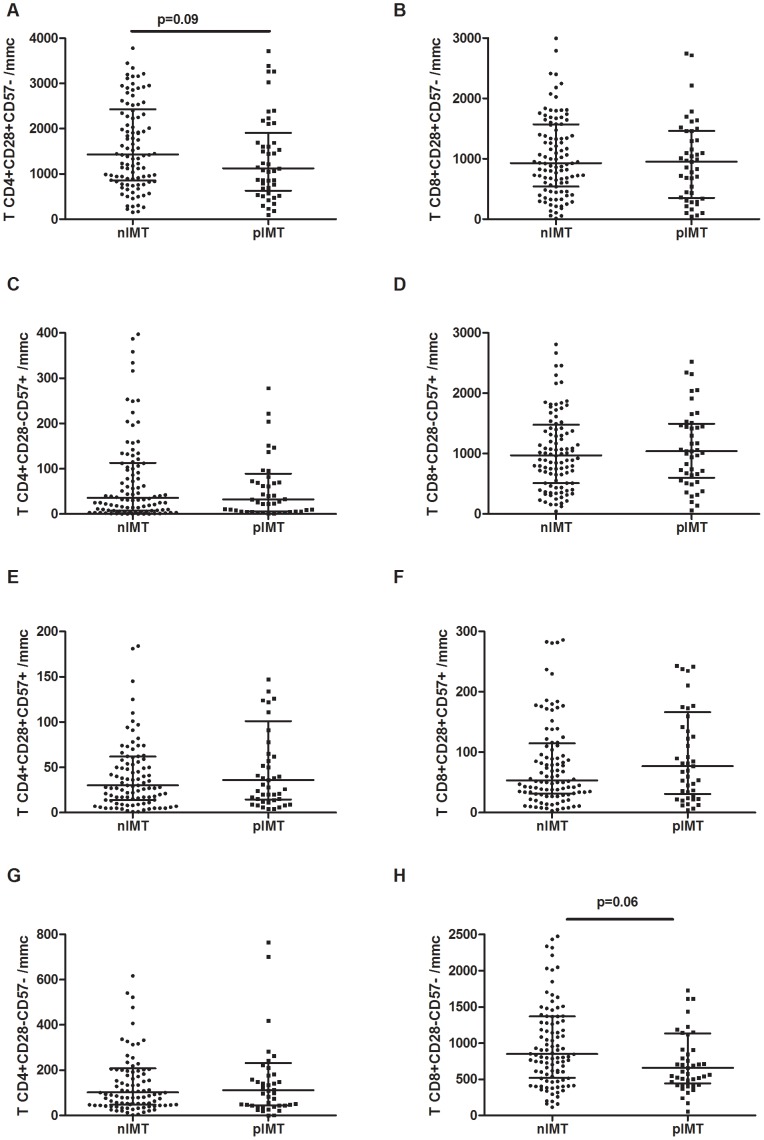
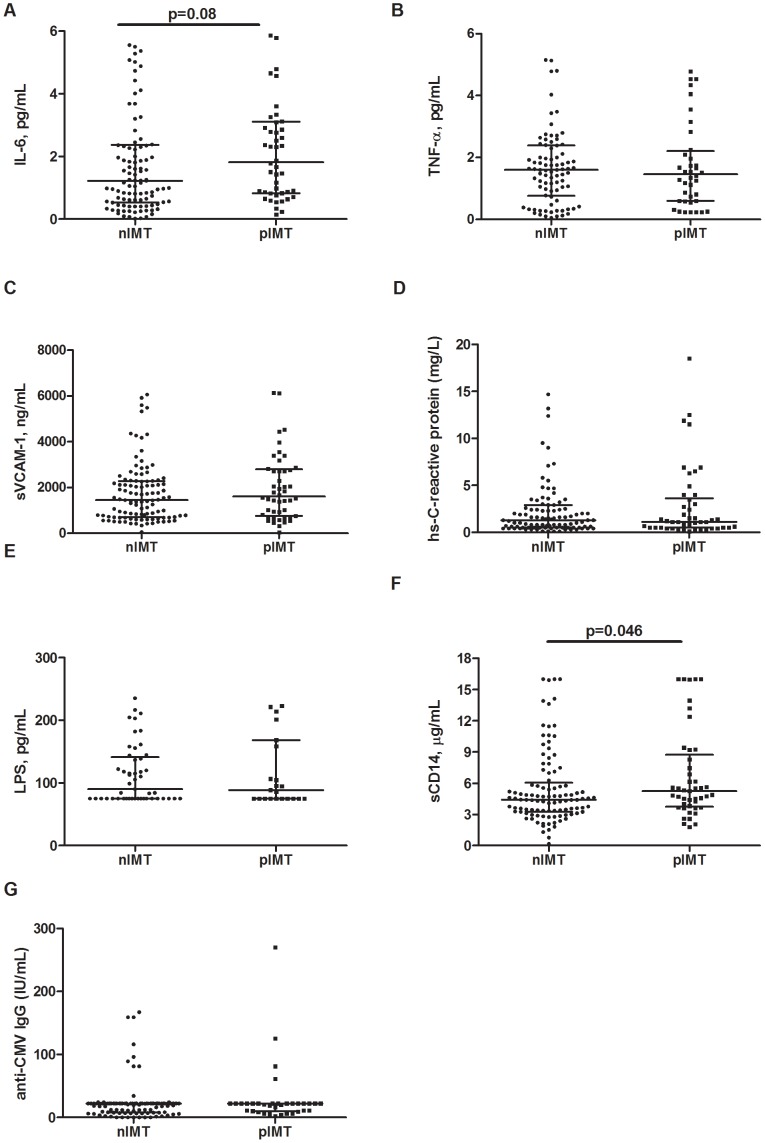
Methods: We measured IMT (carotid ultrasound); CD4+/CD8+ T-cell activation (CD38, CD45R0), differentiation (CD127), apoptosis (CD95), and senescence (CD28, CD57) (flow cytometry); plasma sCD14, IL-6, TNF- α, sVCAM-1, hs-CRP, anti-CMV IgG (ELISA); LPS (LAL). The results were compared by Mann-Whitney, Kruskal-Wallis or Chi-square tests, and factors associated with IMT were evaluated by multivariable logistic regression.
Results: Of 163 patients, 112 demonstrated normal IMT (nIMT), whereas 51 (31.3%) had pathological IMT (pIMT: ≥1 mm). Of the patients with pIMT, 22 demonstrated an increased IMT (iIMT), and 29 were shown to have plaques. These patient groups had comparable nadir and current CD4+, VLs and total length of time on cART. Despite similar proportions of CD38-expressing CD8+ cells (p = .95), pIMT patients exhibited higher activated memory CD8+CD38+CD45R0+ cells (p = .038) and apoptotic CD4+CD95+ (p = .01) and CD8+CD95+ cells (p = .003). In comparison to nIMT patients, iIMT patients tended to have lower numbers of early differentiated CD28+CD57- memory CD4+ (p = .048) and CD28-CD57-CD8+ cells (p = .006), both of which are associated with a higher proliferative potential. Despite no differences in plasma LPS levels, pIMT patients showed significantly higher circulating levels of sCD14 than did nIMT patients (p = .046). No differences in anti-CMV IgG was shown. Although circulating levels of sCD14 seemed to be associated with a risk of ATS in an unadjusted analysis, this effect was lost after adjusting for classical cardiovascular predictors.
Conclusions: Despite the provision of full viral suppression by cART, a hyperactivated, pro-apoptotic T-cell profile characterizes HIV-infected patients with early vascular damage, for whom the potential contribution of subclinical endotoxemia and anti-CMV immunity should be investigated further.
Conflict of interest statement
Figures
References
-
- Savès M, Chêne G, Ducimetière P, Leport C, Le Moal G, et al. (2003) Risk factors for coronary heart disease in patients treated for human immunodeficiency virus infection compared with the general population. Clin Infect Dis 37: 292–298. - PubMed
-
- Friis-Møller N, Reiss P, Sabin CA, Weber R, Monforte A, et al. (2007) Class of antiretroviral drugs and the risk of myocardial infarction. N Engl J Med 356: 1723–1735. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
