

Simple clinical and laboratory predictors of Chikungunya versus dengue infections in adults
- PMID: 23029573
- PMCID: PMC3459852
- DOI: 10.1371/journal.pntd.0001786
Simple clinical and laboratory predictors of Chikungunya versus dengue infections in adults
Abstract
Background: Dengue and chikungunya are co-circulating vector-borne diseases with substantial overlap in clinical presentations. It is important to differentiate between them during first presentation as their management, especially for dengue hemorrhagic fever (DHF), is different. This study compares their clinical presentation in Singapore adults to derive predictors to assist doctors in diagnostic decision-making.
Methods: We compared 117 patients with chikungunya infection diagnosed with reverse transcription-polymerase chain reaction (RT-PCR) with 917 dengue RT-PCR-positive adult patients (including 55 with DHF). We compared dengue fever (DF), DHF, and chikungunya infections by evaluating clinical characteristics of dengue and chikungunya; developing classification tools via multivariate logistic regression models and classification trees of disease etiology using clinical and laboratory factors; and assessing the time course of several clinical variables.
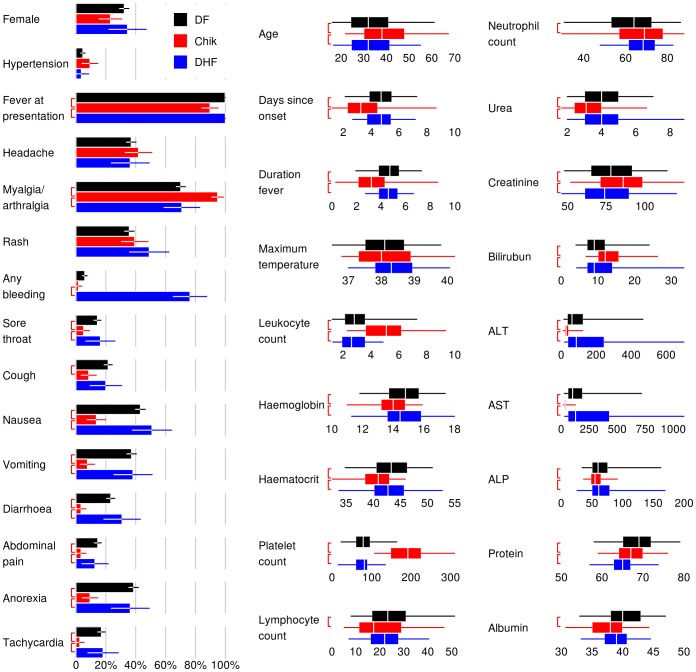
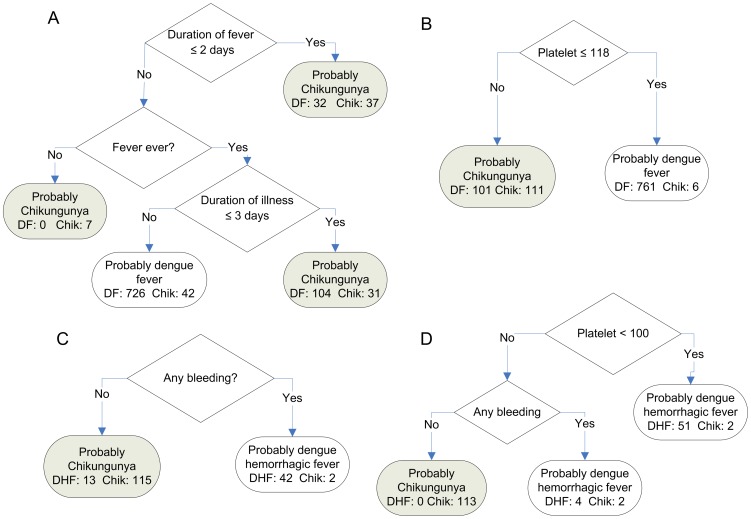
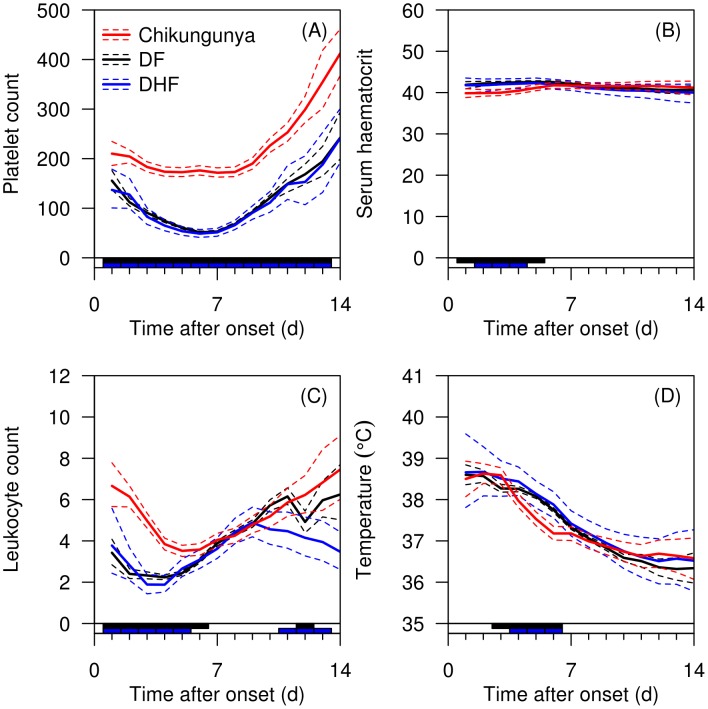
Findings: At first presentation to hospital, significantly more chikungunya patients had myalgia or arthralgia, and fewer had a sore throat, cough (for DF), nausea, vomiting, diarrhea, abdominal pain, anorexia or tachycardia than DF or DHF patients. From the decision trees, platelets <118 × 10(9)/L was the only distinguishing feature for DF versus chikungunya with an overall correct classification of 89%. For DHF versus chikungunya using platelets <100 × 10(9)/L and the presence of bleeding, the overall correct classification was 98%. The time course analysis supported platelet count as the key distinguishing variable.
Interpretation: There is substantial overlap in clinical presentation between dengue and chikungunya infections, but simple clinical and laboratory variables can predict these infections at presentation for appropriate management.
Conflict of interest statement
The authors read the journal's policy and have the following conflicts: VJL received unrelated research funding from GSK. Yee-Sin Leo is a consultant to Sanofi-Pasteur.
Figures
References
-
- World Health Organization (2009) Fact sheet number 117. Dengue and dengue haemorraghic fever. Available: http://www.who.int/mediacentre/factsheets/fs117/en/index.html
-
- World Health Organization (2008) Fact sheet number 327. Chikungunya. Available: http://www.who.int/mediacentre/factsheets/fs327/en/
-
- Pialoux G, Gaüzère BA, Jauréguiberry S, Strobel M (2007) Chikungunya, an epidemic arbovirosis. Lancet Infect Dis 7: 319–327. - PubMed
-
- Staples JE, Breiman RF, Powers AM (2009) Chikungunya fever: an epidemiological review of a re-emerging infectious disease. Clin Infect Dis 49: 942–948. - PubMed
-
- WHO (2009) Dengue: guidelines for diagnosis, treatment, prevention and control. World Health Organization, Geneva. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
