

Dispersion and exposure to a cough-generated aerosol in a simulated medical examination room
- PMID: 23033849
- PMCID: PMC4688889
- DOI: 10.1080/15459624.2012.725986
Dispersion and exposure to a cough-generated aerosol in a simulated medical examination room
Erratum in
-
Correction: J Occup Environ Hyg.2012;9(12):681-90.J Occup Environ Hyg. 2013;10(2):D25. doi: 10.1080/15459624.2013.750545. J Occup Environ Hyg. 2013. PMID: 23259775 No abstract available.
Abstract
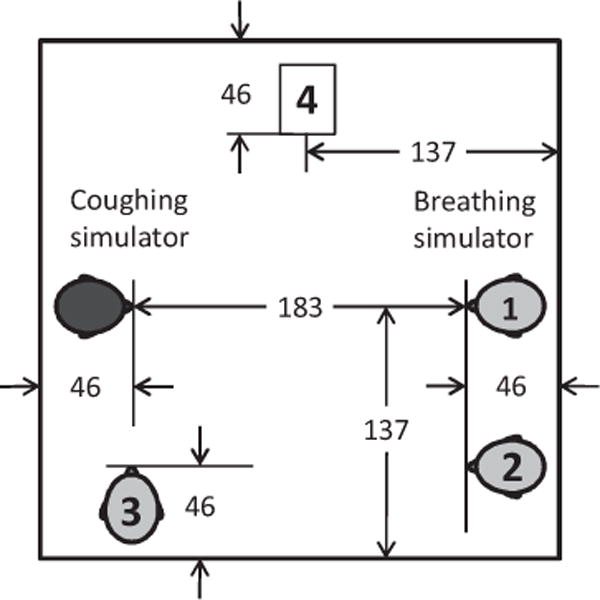
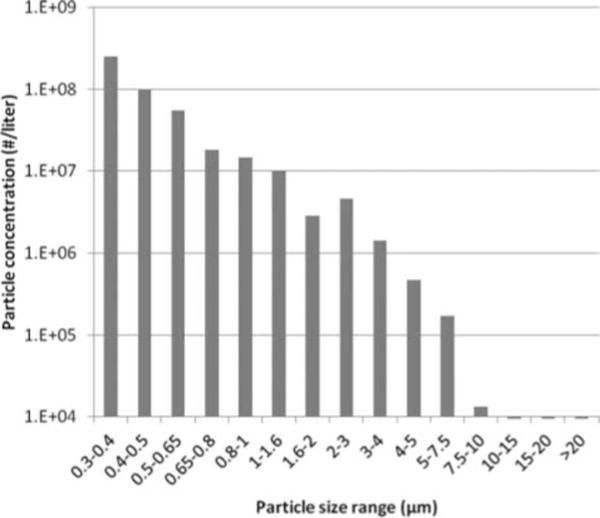
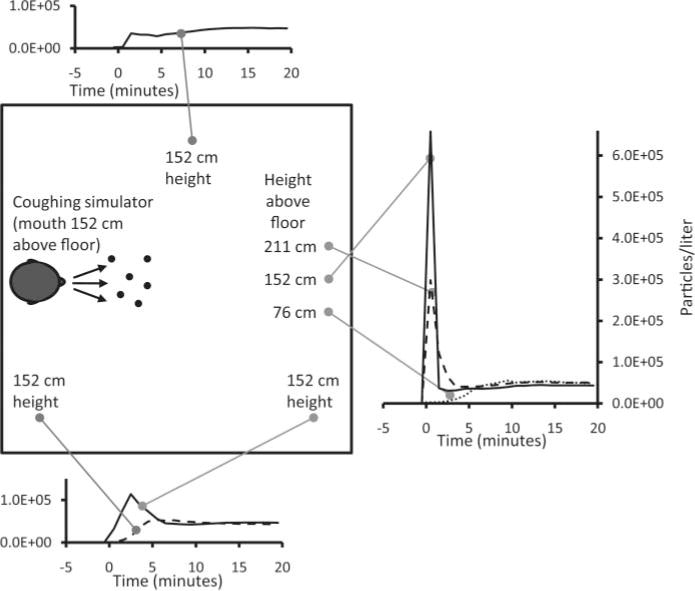
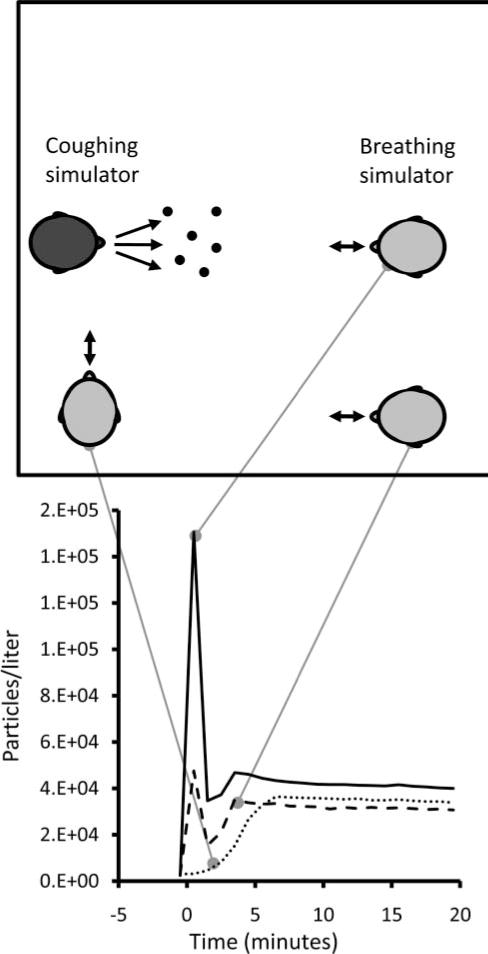
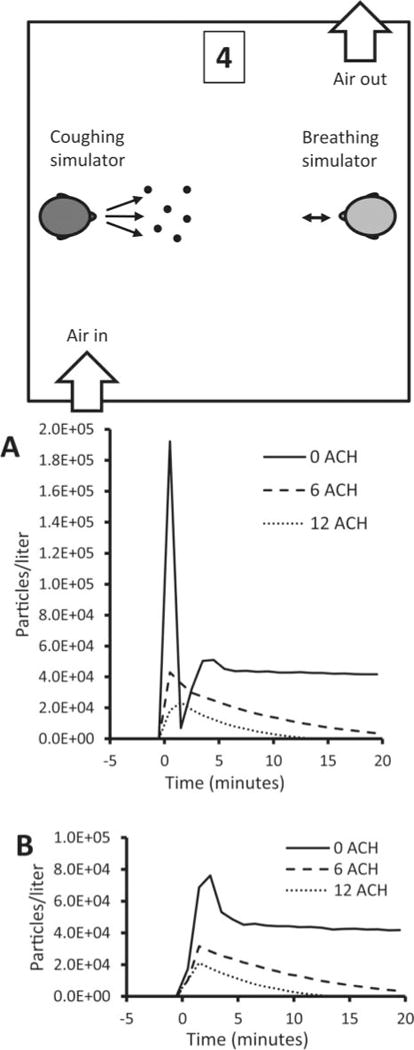
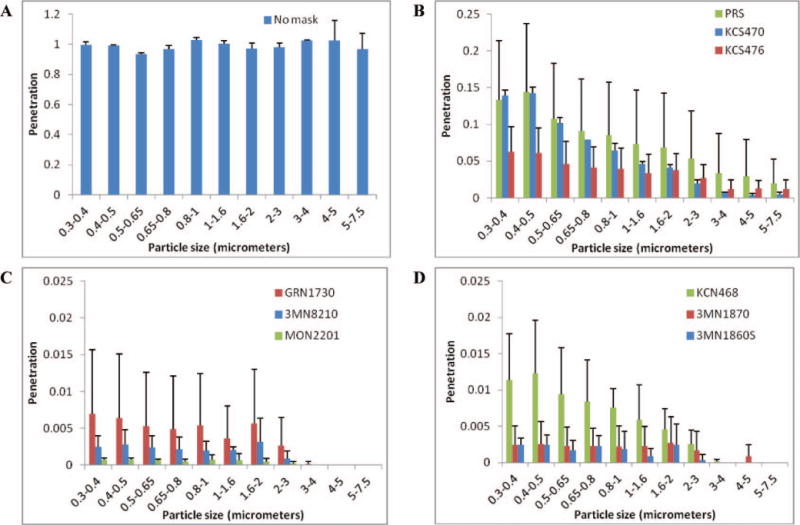
Few studies have quantified the dispersion of potentially infectious bioaerosols produced by patients in the health care environment and the exposure of health care workers to these particles. Controlled studies are needed to assess the spread of bioaerosols and the efficacy of different types of respiratory personal protective equipment (PPE) in preventing airborne disease transmission. An environmental chamber was equipped to simulate a patient coughing aerosol particles into a medical examination room, and a health care worker breathing while exposed to these particles. The system has three main parts: (1) a coughing simulator that expels an aerosol-laden cough through a head form; (2) a breathing simulator with a second head form that can be fitted with respiratory PPE; and (3) aerosol particle counters to measure concentrations inside and outside the PPE and at locations throughout the room. Dispersion of aerosol particles with optical diameters from 0.3 to 7.5 μm was evaluated along with the influence of breathing rate, room ventilation, and the locations of the coughing and breathing simulators. Penetration of cough aerosol particles through nine models of surgical masks and respirators placed on the breathing simulator was measured at 32 and 85 L/min flow rates and compared with the results from a standard filter tester. Results show that cough-generated aerosol particles spread rapidly throughout the room, and that within 5 min, a worker anywhere in the room would be exposed to potentially hazardous aerosols. Aerosol exposure is highest with no personal protective equipment, followed by surgical masks, and the least exposure is seen with N95 FFRs. These differences are seen regardless of breathing rate and relative position of the coughing and breathing simulators. These results provide a better understanding of the exposure of workers to cough aerosols from patients and of the relative efficacy of different types of respiratory PPE, and they will assist investigators in providing research-based recommendations for effective respiratory protection strategies in health care settings.
Figures
References
-
- Li Y, Leung GM, Tang JW, et al. Role of ventilation in airborne transmission of infectious agents in the built environment—A multidisciplinary systematic review. Indoor Air. 2007;17(1):2–18. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical