

C-reactive protein, fibrinogen, and cardiovascular disease prediction
- PMID: 23034020
- PMCID: PMC3714101
- DOI: 10.1056/NEJMoa1107477
C-reactive protein, fibrinogen, and cardiovascular disease prediction
Abstract
Background: There is debate about the value of assessing levels of C-reactive protein (CRP) and other biomarkers of inflammation for the prediction of first cardiovascular events.
Methods: We analyzed data from 52 prospective studies that included 246,669 participants without a history of cardiovascular disease to investigate the value of adding CRP or fibrinogen levels to conventional risk factors for the prediction of cardiovascular risk. We calculated measures of discrimination and reclassification during follow-up and modeled the clinical implications of initiation of statin therapy after the assessment of CRP or fibrinogen.
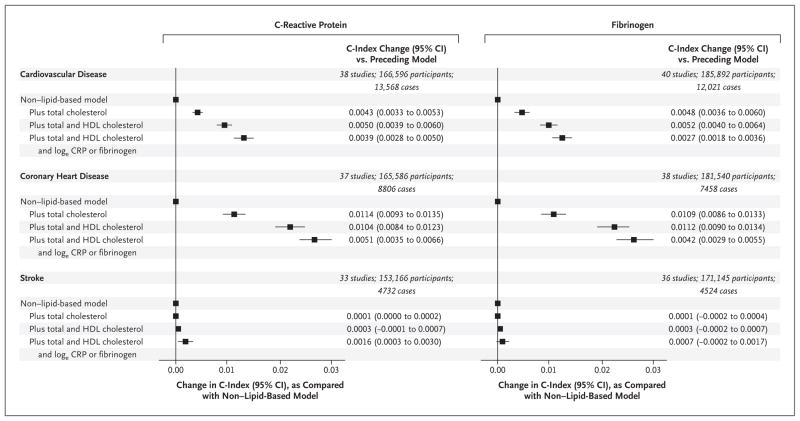
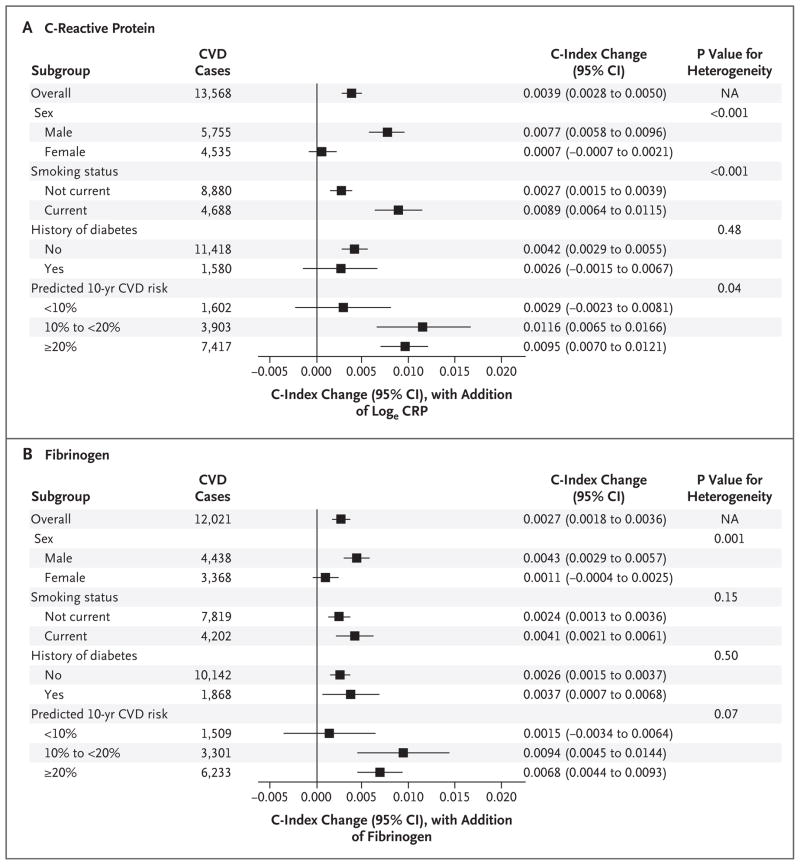
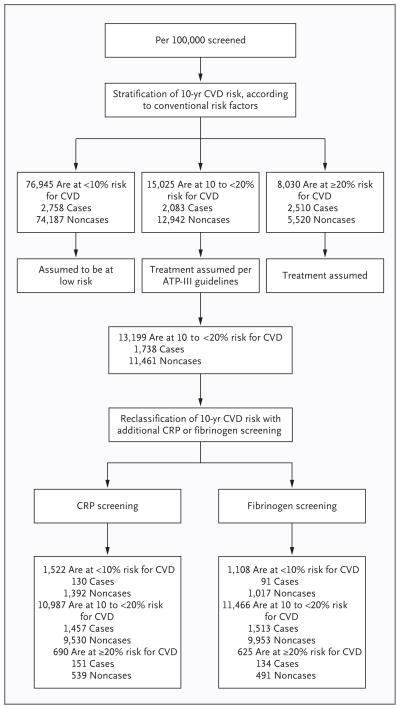
Results: The addition of information on high-density lipoprotein cholesterol to a prognostic model for cardiovascular disease that included age, sex, smoking status, blood pressure, history of diabetes, and total cholesterol level increased the C-index, a measure of risk discrimination, by 0.0050. The further addition to this model of information on CRP or fibrinogen increased the C-index by 0.0039 and 0.0027, respectively (P<0.001), and yielded a net reclassification improvement of 1.52% and 0.83%, respectively, for the predicted 10-year risk categories of "low" (<10%), "intermediate" (10% to <20%), and "high" (≥20%) (P<0.02 for both comparisons). We estimated that among 100,000 adults 40 years of age or older, 15,025 persons would initially be classified as being at intermediate risk for a cardiovascular event if conventional risk factors alone were used to calculate risk. Assuming that statin therapy would be initiated in accordance with Adult Treatment Panel III guidelines (i.e., for persons with a predicted risk of ≥20% and for those with certain other risk factors, such as diabetes, irrespective of their 10-year predicted risk), additional targeted assessment of CRP or fibrinogen levels in the 13,199 remaining participants at intermediate risk could help prevent approximately 30 additional cardiovascular events over the course of 10 years.
Conclusions: In a study of people without known cardiovascular disease, we estimated that under current treatment guidelines, assessment of the CRP or fibrinogen level in people at intermediate risk for a cardiovascular event could help prevent one additional event over a period of 10 years for every 400 to 500 people screened. (Funded by the British Heart Foundation and others.).
Figures
Comment in
-
C-reactive protein, fibrinogen, and cardiovascular risk.N Engl J Med. 2013 Jan 3;368(1):85-6. doi: 10.1056/NEJMc1213688. N Engl J Med. 2013. PMID: 23281988 No abstract available.
-
C-reactive protein, fibrinogen, and cardiovascular risk.N Engl J Med. 2013 Jan 3;368(1):84-5. doi: 10.1056/NEJMc1213688. N Engl J Med. 2013. PMID: 23281989 No abstract available.
-
C-reactive protein, fibrinogen, and cardiovascular risk.N Engl J Med. 2013 Jan 3;368(1):85. doi: 10.1056/NEJMc1213688. N Engl J Med. 2013. PMID: 23281990 No abstract available.
-
C-reactive protein, fibrinogen, and cardiovascular risk.N Engl J Med. 2013 Jan 3;368(1):85. doi: 10.1056/NEJMc1213688. N Engl J Med. 2013. PMID: 23281991 No abstract available.
References
-
- Pearson TA, Mensah GA, Alexander RW, et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation. 2003;107:499–511. - PubMed
-
- Graham I, Atar D, Borch-Johnsen K, et al. European guidelines on cardiovascular disease prevention in clinical practice: executive summary. Eur Heart J. 2007;28:2375–414. - PubMed
-
- Myers GL, Christenson RH, Cushman M, et al. National Academy of Clinical Biochemistry Laboratory Medicine Practice Guidelines: emerging biomarkers for primary prevention of cardiovascular disease. Clin Chem. 2009;55:378–84. - PubMed
-
- Greenland P, Alpert JS, Beller GA, et al. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2010;56(25):e50–e103. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- MC_U137686851/MRC_/Medical Research Council/United Kingdom
- G0600705/MRC_/Medical Research Council/United Kingdom
- G0100222/MRC_/Medical Research Council/United Kingdom
- RG/08/014/24067/BHF_/British Heart Foundation/United Kingdom
- MC_U137686857/MRC_/Medical Research Council/United Kingdom
- P01 HL088117/HL/NHLBI NIH HHS/United States
- MC_U106179471/MRC_/Medical Research Council/United Kingdom
- G0701619/MRC_/Medical Research Council/United Kingdom
- MC_U105260792/MRC_/Medical Research Council/United Kingdom
- RG/08/014/BHF_/British Heart Foundation/United Kingdom
- G19/35/MRC_/Medical Research Council/United Kingdom
- PG/09/002/26056/BHF_/British Heart Foundation/United Kingdom
- G8802774/MRC_/Medical Research Council/United Kingdom
- G1000143/MRC_/Medical Research Council/United Kingdom
- RG/08/013/25942/BHF_/British Heart Foundation/United Kingdom
- G0902037/MRC_/Medical Research Council/United Kingdom
- G0701863/MRC_/Medical Research Council/United Kingdom
- K24 HL084034/HL/NHLBI NIH HHS/United States
- G7900510/MRC_/Medical Research Council/United Kingdom
- R01 HL091099/HL/NHLBI NIH HHS/United States
- MC_U105260558/MRC_/Medical Research Council/United Kingdom
- RG/07/008/23674/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous