

Novel interpretation of molecular diagnosis of congenital toxoplasmosis according to gestational age at the time of maternal infection
- PMID: 23035201
- PMCID: PMC3502944
- DOI: 10.1128/JCM.00918-12
Novel interpretation of molecular diagnosis of congenital toxoplasmosis according to gestational age at the time of maternal infection
Abstract
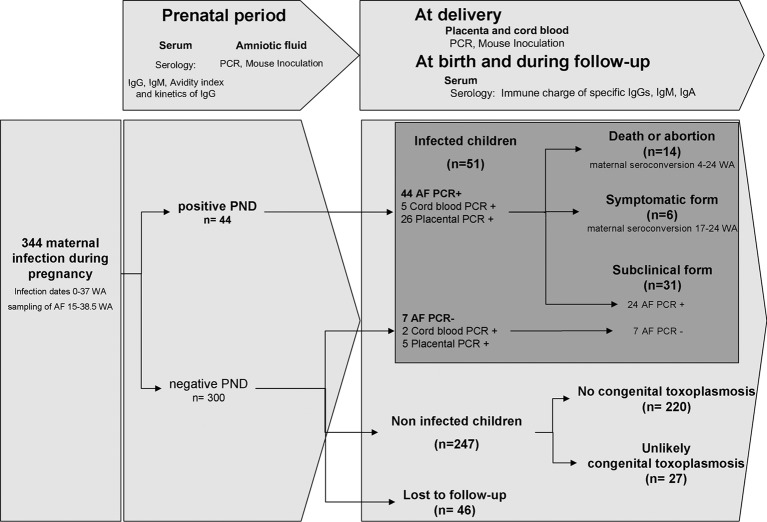
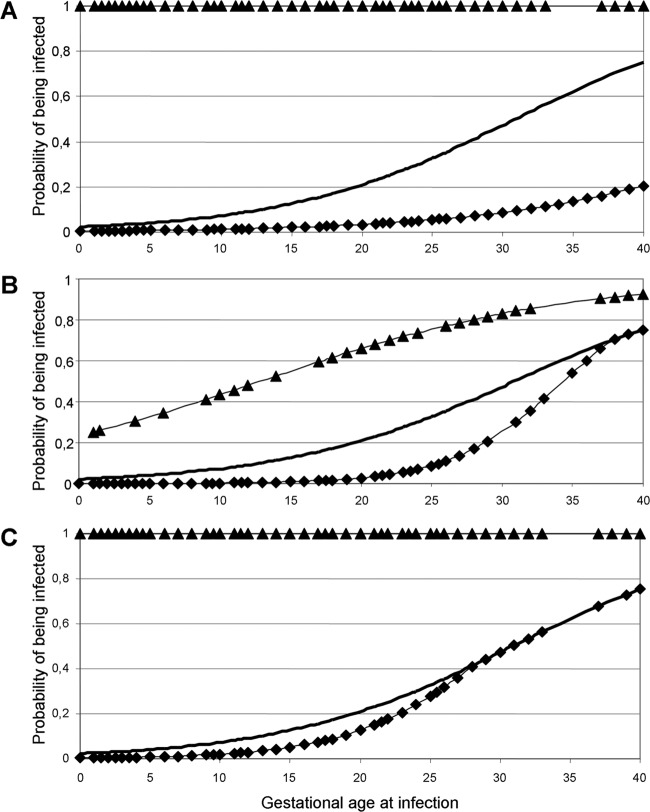
From a prospective cohort of 344 women who seroconverted for toxoplasmosis during pregnancy, 344 amniotic fluid, 264 placenta, and 216 cord blood samples were tested for diagnosis of congenital toxoplasmosis using the same PCR assay. The sensitivity and negative predictive value of the PCR assay using amniotic fluid were 86.3% and 97.2%, respectively, and both specificity and positive predictive value were 100%. Using placenta and cord blood, sensitivities were 79.5% and 21.2%, and specificities were 92% and 100%, respectively. In addition, the calculation of pretest and posttest probabilities and the use of logistic regression allowed us to obtain curves that give a dynamic interpretation of the risk of congenital toxoplasmosis according to gestational age at maternal infection, as represented by the three sample types (amniotic fluid, placenta, and cord blood). Two examples are cited here: for a maternal infection at 25 weeks of amenorrhea, a negative result of prenatal diagnosis allowed estimation of the probability of congenital toxoplasmosis at 5% instead of an a priori (pretest) risk estimate of 33%. For an infection at 10 weeks of amenorrhea associated with a pretest congenital toxoplasmosis risk of 7%, a positive PCR result using placenta at birth yields a risk increase to 43%, while a negative result damps down the risk to 0.02%. Thus, with a molecular diagnosis performing at a high level, and in spite of the persistence of false negatives, posttest risk curves using both negative and positive results prove highly informative, allowing a better assessment of the actual risk of congenital toxoplasmosis and finally an improved decision guide to treatment.
Figures
References
-
- Ajzenberg D, et al. 2002. Genotype of 86 Toxoplasma gondii isolates associated with human congenital toxoplasmosis, and correlation with clinical findings. J. Infect. Dis. 186:684–689 - PubMed
-
- Anonymous 1992. Congenital toxoplasmosis, Copenhagen, January 17, 1992. Proceedings. Scand. J. Infect. Dis. Suppl. 84:1–96 - PubMed
-
- Bastien P. 2002. Molecular diagnosis of toxoplasmosis. Trans. R. Soc. Trop. Med. Hyg. 96(Suppl 1):S205–S215 - PubMed
-
- Berger F, Goulet G, Le Strat Y, Desenclos J. 2008. Toxoplasmosis in pregnant women in France: trends in seroprevalence and incidence, and associated factors, 1995–2003. Bull. Epidémiol. Hebdomadaire 14-15:117–121 (In French.)
-
- Bessieres MH, et al. 2009. Diagnosis of congenital toxoplasmosis: prenatal and neonatal evaluation of methods used in Toulouse University Hospital and incidence of congenital toxoplasmosis. Mem. Inst. Oswaldo Cruz 104:389–392 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
