

Use of multiple imputation method to improve estimation of missing baseline serum creatinine in acute kidney injury research
- PMID: 23037980
- PMCID: PMC3531649
- DOI: 10.2215/CJN.00200112
Use of multiple imputation method to improve estimation of missing baseline serum creatinine in acute kidney injury research
Abstract
Background and objectives: Baseline creatinine (BCr) is frequently missing in AKI studies. Common surrogate estimates can misclassify AKI and adversely affect the study of related outcomes. This study examined whether multiple imputation improved accuracy of estimating missing BCr beyond current recommendations to apply assumed estimated GFR (eGFR) of 75 ml/min per 1.73 m(2) (eGFR 75).
Design, setting, participants, & measurements: From 41,114 unique adult admissions (13,003 with and 28,111 without BCr data) at Vanderbilt University Hospital between 2006 and 2008, a propensity score model was developed to predict likelihood of missing BCr. Propensity scoring identified 6502 patients with highest likelihood of missing BCr among 13,003 patients with known BCr to simulate a "missing" data scenario while preserving actual reference BCr. Within this cohort (n=6502), the ability of various multiple-imputation approaches to estimate BCr and classify AKI were compared with that of eGFR 75.
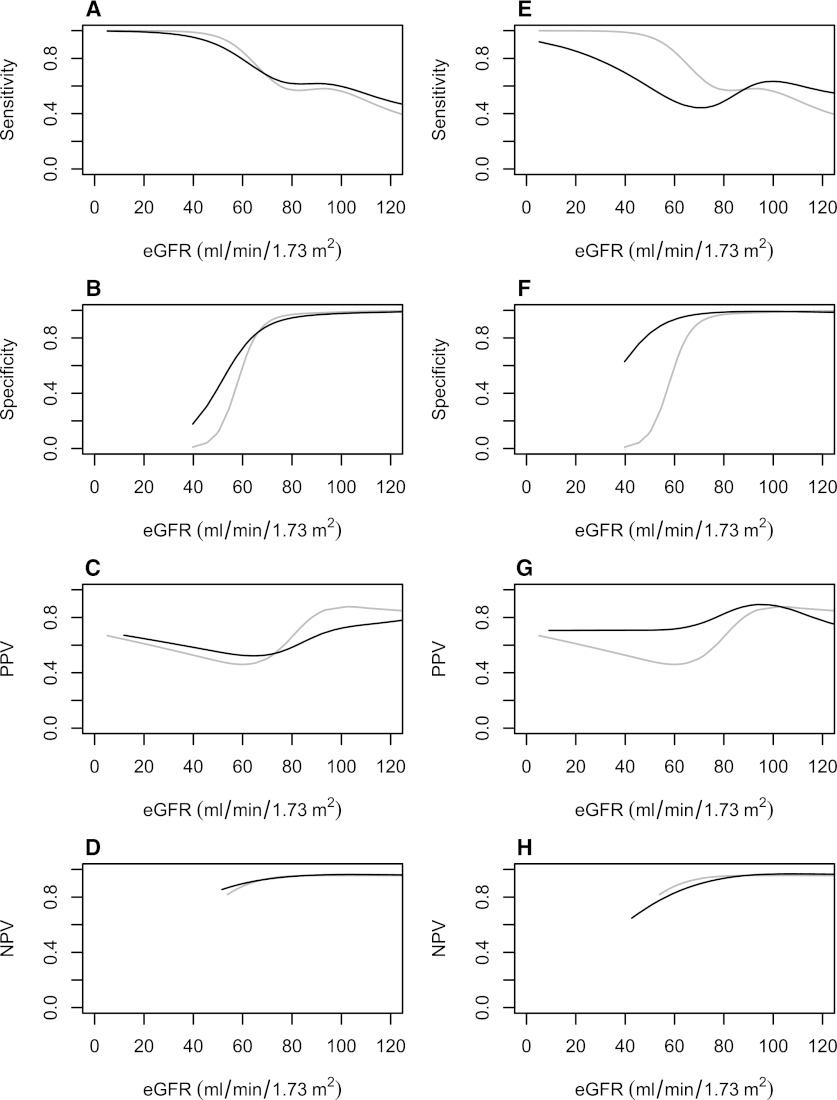
Results: All multiple-imputation methods except the basic one more closely approximated actual BCr than did eGFR 75. Total AKI misclassification was lower with multiple imputation (full multiple imputation + serum creatinine) (9.0%) than with eGFR 75 (12.3%; P<0.001). Improvements in misclassification were greater in patients with impaired kidney function (full multiple imputation + serum creatinine) (15.3%) versus eGFR 75 (40.5%; P<0.001). Multiple imputation improved specificity and positive predictive value for detecting AKI at the expense of modestly decreasing sensitivity relative to eGFR 75.
Conclusions: Multiple imputation can improve accuracy in estimating missing BCr and reduce misclassification of AKI beyond currently proposed methods.
Figures

References
-
- Xue JL, Daniels F, Star RA, Kimmel PL, Eggers PW, Molitoris BA, Himmelfarb J, Collins AJ: Incidence and mortality of acute renal failure in Medicare beneficiaries, 1992 to 2001. J Am Soc Nephrol 17: 1135–1142, 2006 - PubMed
-
- Bagshaw SM, Uchino S, Cruz D, Bellomo R, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A, Oudemans-van Straaten HM, Ronco C, Kellum JA, Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators : A comparison of observed versus estimated baseline creatinine for determination of RIFLE class in patients with acute kidney injury. Nephrol Dial Transplant 24: 2739–2744, 2009 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
