

Patella re-alignment in children with a modified Grammont technique
- PMID: 23039166
- PMCID: PMC3488178
- DOI: 10.3109/17453674.2012.736168
Patella re-alignment in children with a modified Grammont technique
Abstract
Background and purpose: In skeletally immature patients, surgical options due to recurrent patella dislocation are limited, because bony procedures bear the risk of growth disturbances. In this retrospective study, we report the long-term functional and radiographic outcome in skeletally immature patients using the modified Grammont surgical technique.
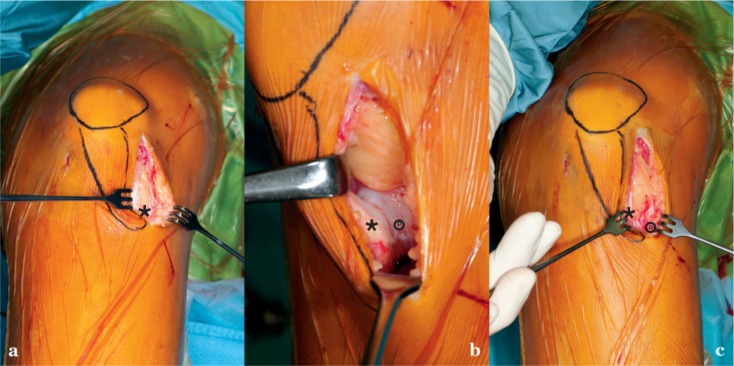
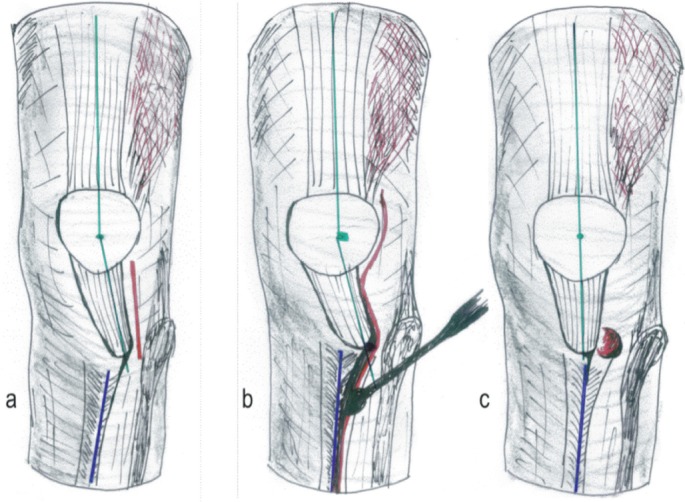
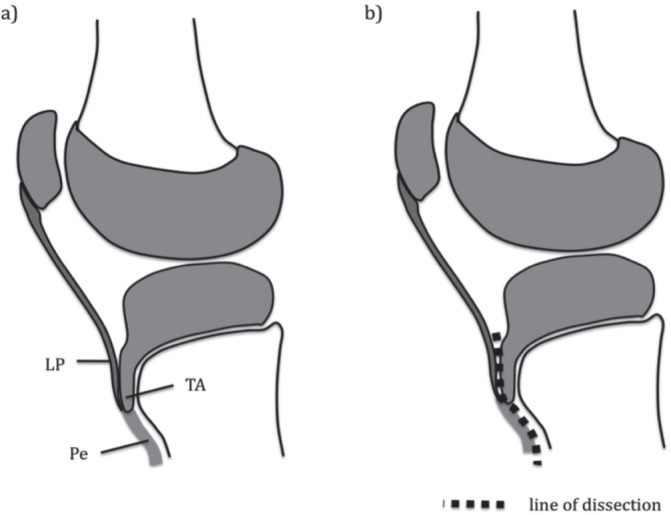
Patients: Between 1999 and 2004, 65 skeletally immature knees (49 children) were treated with a modified Grammont procedure: an open lateral release and a shift of the patella tendon insertion below the growth plate on the tuberositas tibia, allowing the tendon to medialize. At mean 8 (5.6-11) years after surgery, 58 knees in 43 patients were evaluated by clinical examination, from functional scores (Lysholm, Tegner), and from radiographs of the knees.
Results: Mean Lysholm score was 82 postoperatively. Tegner score decreased from 6.2 to 5. Eight knees had a single dislocation within 3 months of surgery. 3 knees had repeated late dislocations, all with a high grade of trochlea dysplasia. 6 knees showed mild signs of osteoarthritis. No growth disturbances were observed.
Interpretation: The modified Grammont technique in skeletally immature patients allows restoration of the distal patella tendon alignment by dynamic positioning. Long-term results showed that there were no growth disturbances and that there was good functional outcome. However, patients with a high grade of trochlea dysplasia tended to re-dislocate.
Figures
References
-
- Airanow S, Zippel H. Femoro-tibial torsion in patellar instability. A contribution to the pathogenesis of recurrent and habitual patellar dislocations. Beitr Orthop Traumatol. 1990;37(6):311–6. - PubMed
-
- Ali S, Bhatti A. Arthroscopic proximal realignment of the patella for recurrent instability: report of a new surgical technique with 1 to 7 years of follow-up. Arthroscopy. 2007;23(3):305–11. - PubMed
-
- Arendt EA, Fithian DC, Cohen E. Current concepts of lateral patella dislocation. Clin Sports Med. 2002;21(3):499–519. - PubMed
-
- Arnbjornsson A, Egund N, Rydling O, Stockerup R, Ryd L. The natural history of recurrent dislocation of the patella. Long-term results of conservative and operative treatment. J Bone Joint Surg (Br) 1992;74(1):140–2. - PubMed
-
- Barber FA, McGarry JE. Patterns of hip rotation range of motion: a comparison between healthy subjects and patients with low back pain. Phys Ther. 1990;70:537–41. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources