

Screening for type 2 diabetes and population mortality over 10 years (ADDITION-Cambridge): a cluster-randomised controlled trial
- PMID: 23040422
- PMCID: PMC3607818
- DOI: 10.1016/S0140-6736(12)61422-6
Screening for type 2 diabetes and population mortality over 10 years (ADDITION-Cambridge): a cluster-randomised controlled trial
Abstract
Background: The increasing prevalence of type 2 diabetes poses a major public health challenge. Population-based screening and early treatment for type 2 diabetes could reduce this growing burden. However, uncertainty persists around the benefits of screening for type 2 diabetes. We assessed the effect of a population-based stepwise screening programme on mortality.
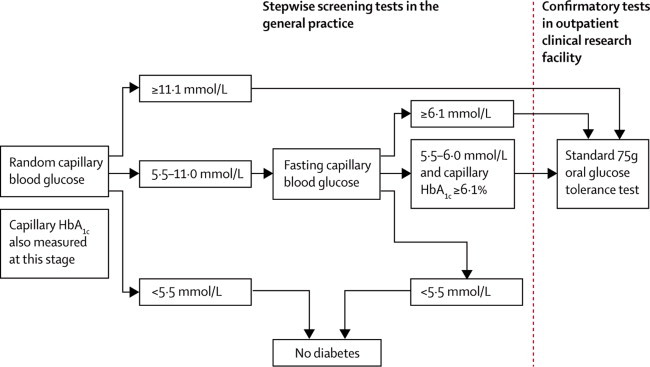
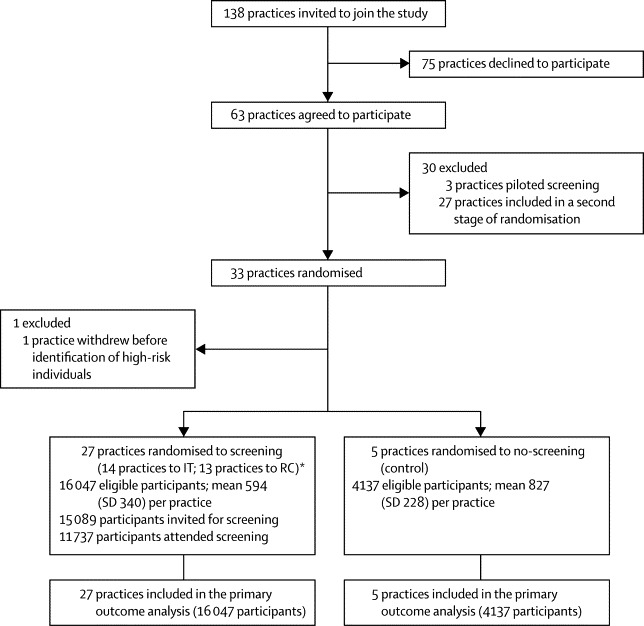
Methods: In a pragmatic parallel group, cluster-randomised trial, 33 general practices in eastern England were randomly assigned by the method of minimisation in an unbalanced design to: screening followed by intensive multifactorial treatment for people diagnosed with diabetes (n=15); screening plus routine care of diabetes according to national guidelines (n=13); and a no-screening control group (n=5). The study population consisted of 20,184 individuals aged 40-69 years (mean 58 years), at high risk of prevalent undiagnosed diabetes, on the basis of a previously validated risk score. In screening practices, individuals were invited to a stepwise programme including random capillary blood glucose and glycated haemoglobin (HbA(1c)) tests, a fasting capillary blood glucose test, and a confirmatory oral glucose tolerance test. The primary outcome was all-cause mortality. All participants were flagged for mortality surveillance by the England and Wales Office of National Statistics. Analysis was by intention-to-screen and compared all-cause mortality rates between screening and control groups. This study is registered, number ISRCTN86769081.
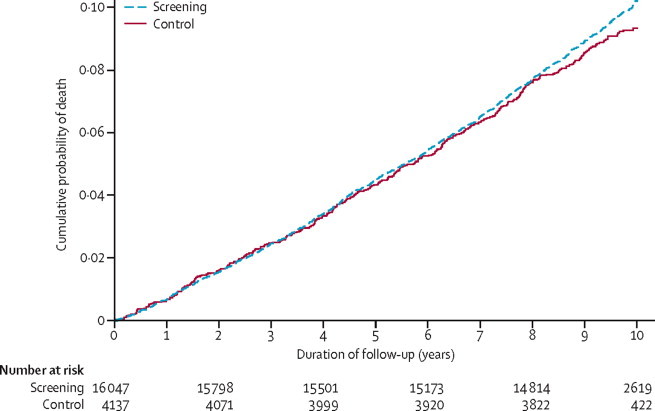
Findings: Of 16,047 high-risk individuals in screening practices, 15,089 (94%) were invited for screening during 2001-06, 11,737 (73%) attended, and 466 (3%) were diagnosed with diabetes. 4137 control individuals were followed up. During 184,057 person-years of follow up (median duration 9·6 years [IQR 8·9-9·9]), there were 1532 deaths in the screening practices and 377 in control practices (mortality hazard ratio [HR] 1·06, 95% CI 0·90-1·25). We noted no significant reduction in cardiovascular (HR 1·02, 95% CI 0·75-1·38), cancer (1·08, 0·90-1·30), or diabetes-related mortality (1·26, 0·75-2·10) associated with invitation to screening.
Interpretation: In this large UK sample, screening for type 2 diabetes in patients at increased risk was not associated with a reduction in all-cause, cardiovascular, or diabetes-related mortality within 10 years. The benefits of screening might be smaller than expected and restricted to individuals with detectable disease.
Funding: Wellcome Trust; UK Medical Research Council; National Health Service research and development support; UK National Institute for Health Research; University of Aarhus, Denmark; Bio-Rad.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Tackling the global diabetes burden: will screening help?Lancet. 2012 Nov 17;380(9855):1716-8. doi: 10.1016/S0140-6736(12)61682-1. Epub 2012 Oct 4. Lancet. 2012. PMID: 23040423 No abstract available.
-
Diabetes: screening for T2DM does not reduce mortality.Nat Rev Endocrinol. 2012 Dec;8(12):694. doi: 10.1038/nrendo.2012.200. Epub 2012 Oct 23. Nat Rev Endocrinol. 2012. PMID: 23090207 No abstract available.
-
ACP Journal Club. A single screening for type 2 diabetes in high-risk adults did not reduce mortality over 10 years.Ann Intern Med. 2013 Jan 15;158(2):JC4. doi: 10.7326/0003-4819-158-2-201301150-02004. Ann Intern Med. 2013. PMID: 23318338 No abstract available.
-
Screening for type 2 diabetes does not reduce mortality over 10 years.Evid Based Med. 2013 Oct;18(5):e44. doi: 10.1136/eb-2012-101186. Epub 2013 Feb 22. Evid Based Med. 2013. PMID: 23435254 No abstract available.
-
Screening for type 2 diabetes and population mortality over 10 years.Lancet. 2013 Mar 16;381(9870):901-2. doi: 10.1016/S0140-6736(13)60665-0. Lancet. 2013. PMID: 23499033 No abstract available.
-
Screening for type 2 diabetes and population mortality over 10 years.Lancet. 2013 Mar 16;381(9870):902-3. doi: 10.1016/S0140-6736(13)60667-4. Lancet. 2013. PMID: 23499034 No abstract available.
-
Screening for type 2 diabetes and population mortality over 10 years.Lancet. 2013 Mar 16;381(9870):902. doi: 10.1016/S0140-6736(13)60666-2. Lancet. 2013. PMID: 23499035 No abstract available.
-
Screening for type 2 diabetes and population mortality over 10 years - authors' reply.Lancet. 2013 Mar 16;381(9870):903. doi: 10.1016/S0140-6736(13)60668-6. Lancet. 2013. PMID: 23499036 No abstract available.
References
-
- Simmons RK, Echouffo-Tcheugui JB, Griffin SJ. Screening for type 2 diabetes: an update of the evidence. Diabetes Obes Metab. 2010;12:838–844. - PubMed
-
- Department of Health . Putting prevention first. Vascular checks: risk assessment and management. Department of Health; London: 2008.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
