

Mutations in calmodulin cause ventricular tachycardia and sudden cardiac death
- PMID: 23040497
- PMCID: PMC3484646
- DOI: 10.1016/j.ajhg.2012.08.015
Mutations in calmodulin cause ventricular tachycardia and sudden cardiac death
Abstract
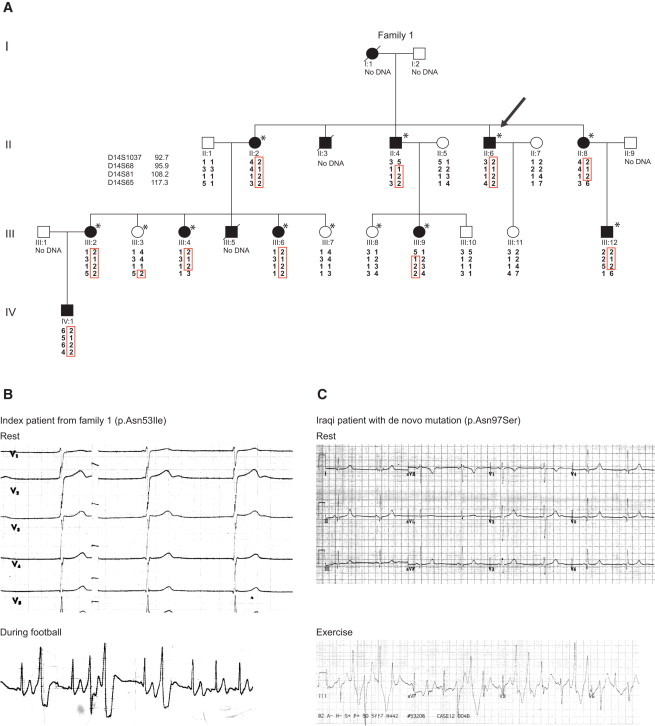
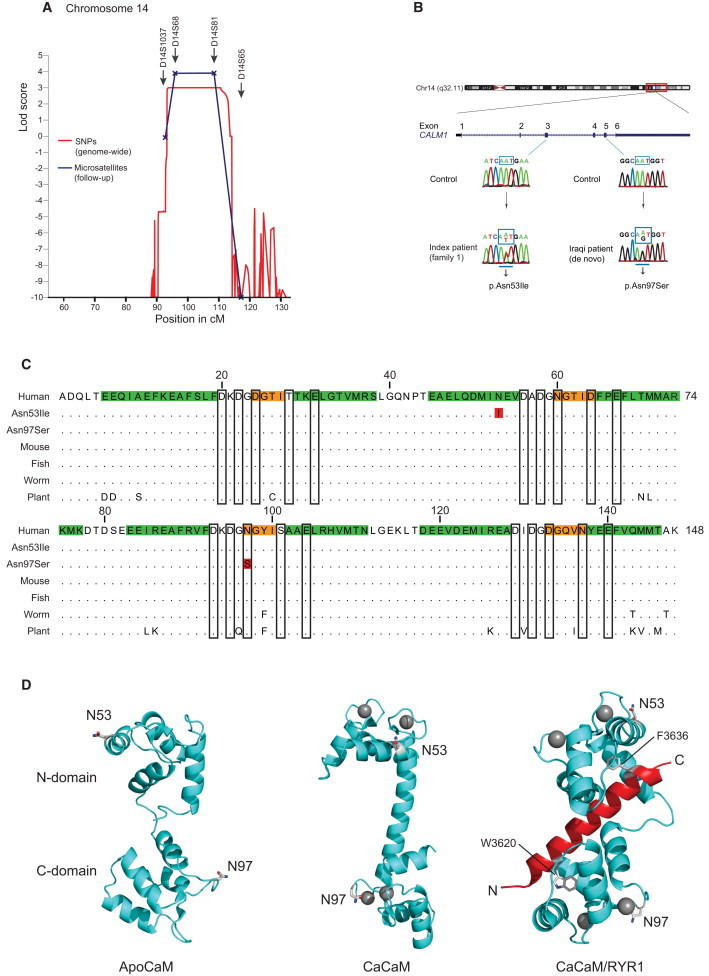
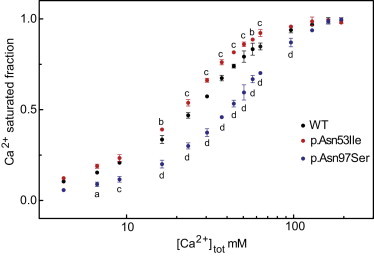
Catecholaminergic polymorphic ventricular tachycardia (CPVT) is a devastating inherited disorder characterized by episodic syncope and/or sudden cardiac arrest during exercise or acute emotion in individuals without structural cardiac abnormalities. Although rare, CPVT is suspected to cause a substantial part of sudden cardiac deaths in young individuals. Mutations in RYR2, encoding the cardiac sarcoplasmic calcium channel, have been identified as causative in approximately half of all dominantly inherited CPVT cases. Applying a genome-wide linkage analysis in a large Swedish family with a severe dominantly inherited form of CPVT-like arrhythmias, we mapped the disease locus to chromosome 14q31-32. Sequencing CALM1 encoding calmodulin revealed a heterozygous missense mutation (c.161A>T [p.Asn53Ile]) segregating with the disease. A second, de novo, missense mutation (c.293A>G [p.Asn97Ser]) was subsequently identified in an individual of Iraqi origin; this individual was diagnosed with CPVT from a screening of 61 arrhythmia samples with no identified RYR2 mutations. Both CALM1 substitutions demonstrated compromised calcium binding, and p.Asn97Ser displayed an aberrant interaction with the RYR2 calmodulin-binding-domain peptide at low calcium concentrations. We conclude that calmodulin mutations can cause severe cardiac arrhythmia and that the calmodulin genes are candidates for genetic screening of individual cases and families with idiopathic ventricular tachycardia and unexplained sudden cardiac death.
Copyright © 2012 The American Society of Human Genetics. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Badhwar N., Scheinman M.M. Idiopathic ventricular tachycardia: Diagnosis and management. Curr. Probl. Cardiol. 2007;32:7–43. - PubMed
-
- Coumel P., Fidelle J., Lucet V., Attuel P., Bouvrain Y. Catecholaminergic-induced severe ventricular arrhythmias with Adams-Stokes syndrome in children: Report of four cases. Br. Heart J. 1978;40(suppl):28–37.
-
- Napolitano C., Priori S.G. Diagnosis and treatment of catecholaminergic polymorphic ventricular tachycardia. Heart Rhythm. 2007;4:675–678. - PubMed
-
- Aizawa Y., Komura S., Okada S., Chinushi M., Aizawa Y., Morita H., Ohe T. Distinct U wave changes in patients with catecholaminergic polymorphic ventricular tachycardia (CPVT) Int. Heart J. 2006;47:381–389. - PubMed
-
- Viitasalo M., Oikarinen L., Väänänen H., Kontula K., Toivonen L., Swan H. U-waves and T-wave peak to T-wave end intervals in patients with catecholaminergic polymorphic ventricular tachycardia, effects of beta-blockers. Heart Rhythm. 2008;5:1382–1388. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
