

Microcystic macular oedema, thickness of the inner nuclear layer of the retina, and disease characteristics in multiple sclerosis: a retrospective study
- PMID: 23041237
- PMCID: PMC3533139
- DOI: 10.1016/S1474-4422(12)70213-2
Microcystic macular oedema, thickness of the inner nuclear layer of the retina, and disease characteristics in multiple sclerosis: a retrospective study
Erratum in
- Lancet Neurol. 2012 Dec;11(12):1021
Abstract
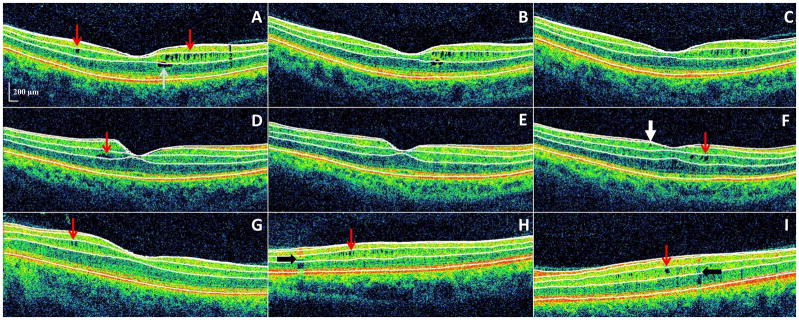
Background: Microcystic macular oedema (MMO) of the retinal inner nuclear layer (INL) has been identified in patients with multiple sclerosis (MS) by use of optical coherence tomography (OCT). We aimed to determine whether MMO of the INL, and increased thickness of the INL are associated with disease activity or disability progression.
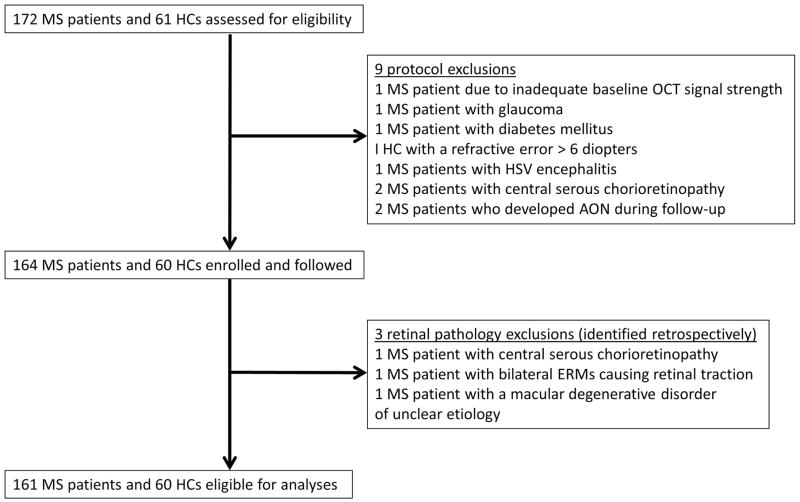
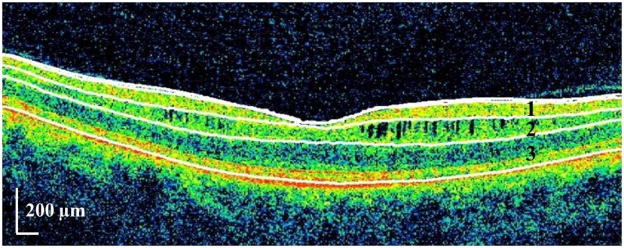
Methods: This retrospective study was done at the Johns Hopkins Hospital (Baltimore, MD, USA), between September, 2008, and March, 2012. Patients with MS and healthy controls underwent serial OCT scans and clinical assessments including visual function. OCT scanning, including automated intraretinal layer segmentation, yielded thicknesses of the retinal nerve fibre layer, the ganglion cell layer plus inner plexiform layer, the INL plus outer plexiform layer (the combined thickness of these layers was used as a surrogate measure of INL thickness), and the outer nuclear layer. Patients with MS also underwent annual brain MRI scans. Disability scores were compared with the Wilcoxon rank-sum test. Mixed-effects linear regression was used to compare OCT measures and letter-acuity scores. Logistic regression was used to examine the relations of baseline OCT thicknesses with clinical and radiological parameters.
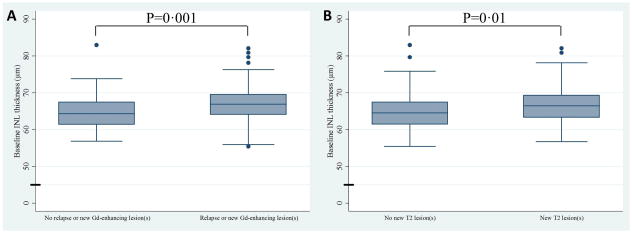
Findings: 164 patients with MS and 60 healthy controls were assessed. Mean follow-up was 25·8 months (SD 9·1) for patients with MS and 22·4 months (11·4) for healthy controls. Ten (6%) patients with MS had MMO during at least one study visit; MMO was visible at baseline in four of these patients. Healthy controls did not have MMO. Patients with MS and MMO had higher baseline MS severity scores (median 5·93 [range 2·44-8·91]) than those who did not have MMO at any time during the study (151 patients; 3·81 [0·13-9·47]; p=0·032), although expanded disability status scale (EDSS) scores were not significantly different (5·2 [1·0-6·5] for patients with MS and MMO vs 2·5 [0·0-8·0] for those without MMO; p=0·097). The eyes of patients with MS and MMO (12 eyes) versus those without MMO (302 eyes) had lower letter-acuity scores (100% contrast, p=0·017; 2·5% contrast, p=0·031; 1·25% contrast, p=0·014), and increased INL thicknesses (p=0·003) at baseline. Increased baseline INL thickness in patients with MS was associated with the development of contrast-enhancing lesions (p=0·007), new T2 lesions (p=0·015), EDSS progression (p=0·034), and relapses in patients with relapsing-remitting MS (p=0·008) during the study. MMO was not associated with disease activity during follow-up.
Interpretation: Increased INL thickness on OCT is associated with disease activity in MS. If this finding is confirmed, INL thickness could be a useful predictor of disease progression in patients with MS.
Funding: National Multiple Sclerosis Society, National Eye Institute, Braxton Debbie Angela Dillon and Skip Donor Advisor Fund.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Conflict of interest statement
We declare that we have no conflicts of interest
Figures
Comment in
-
Microcystic macular oedema in MS: T2 lesion or black hole?Lancet Neurol. 2012 Nov;11(11):933-4. doi: 10.1016/S1474-4422(12)70231-4. Epub 2012 Oct 4. Lancet Neurol. 2012. PMID: 23041238 No abstract available.
References
-
- Prineas J. Pathology of multiple sclerosis. In: Cook S, editor. Handbook of multiple sclerosis. New York: Marcel Dekker; 2001. pp. 289–324.
-
- Calabrese M, Atzori M, Bernardi V, et al. Cortical atrophy is relevant in multiple sclerosis at clinical onset. J Neurol. 2007;254(9):1212–1220. - PubMed
-
- Calabrese M, Agosta F, Rinaldi F, et al. Cortical lesions and atrophy associated with cognitive impairment in relapsing-remitting multiple sclerosis. Arch Neurol. 2009;66(9):1144–1150. - PubMed
-
- Moll NM, Rietsch AM, Ransohoff AJ, et al. Cortical demyelination in PML and MS: Similarities and differences. Neurology. 2008;70(5):336–343. - PubMed
-
- Saidha S, Syc SB, Ibrahim MA, et al. Primary retinal pathology in multiple sclerosis as detected by optical coherence tomography. Brain. 2011;134(Pt 2):518–533. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
