

Transplantation conditioning regimens and outcomes after allogeneic hematopoietic cell transplantation in children and adolescents with acute lymphoblastic leukemia
- PMID: 23041605
- PMCID: PMC3553255
- DOI: 10.1016/j.bbmt.2012.09.019
Transplantation conditioning regimens and outcomes after allogeneic hematopoietic cell transplantation in children and adolescents with acute lymphoblastic leukemia
Abstract
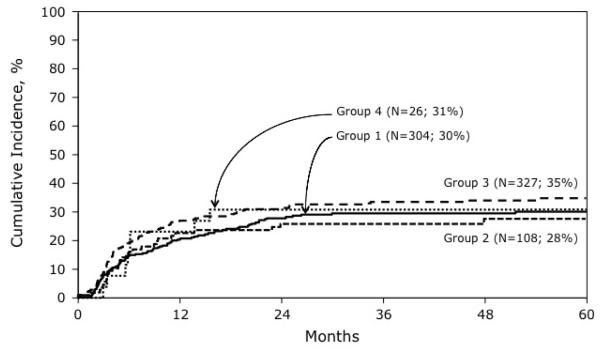
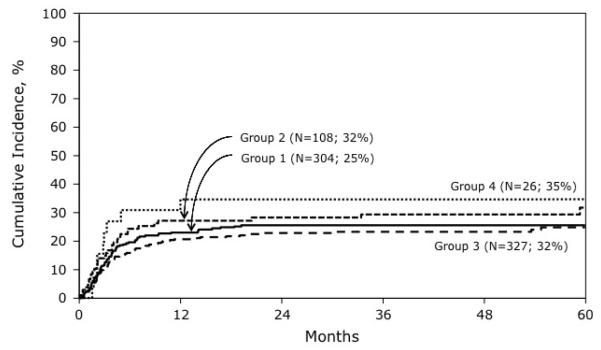
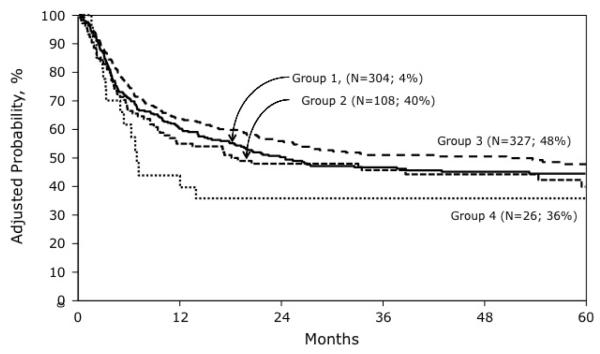
Relapse is common after hematopoietic stem cell transplantation (HSCT) for acute lymphoblastic leukemia (ALL). Although 1200 cGy total body irradiation (TBI) and cyclophosphamide (Cy) is the standard conditioning regimen, attempts to reduce relapse have led to the addition of a second chemotherapeutic agent and/or higher dose of TBI. We examined HSCT outcomes in patients age <18 years with ALL, in second or subsequent remission or in relapse at transplantation. Most transplantations were performed with the patient in remission. Patients received grafts from an HLA-matched sibling or unrelated donor. Four treatment groups were created: (1) Cy + TBI ≤ 1200 cGy (n = 304), (2) Cy + etoposide + TBI ≤ 1200 cGy (n = 108), (3) Cy + TBI ≥ 1300 cGy (n = 327), and (4) Cy + etoposide + TBI ≥ 1300 cGy (n = 26). Neither TBI > 1200 cGy nor the addition of etoposide resulted in fewer relapses. The 5-year probability of relapse was 30% for group 1, 28% for group 2, 35% for group 3, and 31% for group 4. However, transplantation-related mortality was higher (35% versus 25%, P = .02) and overall survival lower (36% versus 48%, P = .03) in group 4 compared with group 3. Our findings indicate that compared with the standard regimen, neither TBI > 1200 cGy nor the addition of etoposide improves survival after HSCT for ALL.
Copyright © 2013 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Chessells JM. The management of high-risk lymphoblastic leukaemia in children. Br J Haematol. 2000;108:204–216. - PubMed
-
- Borgmann A, von Stackelberg A, Hartmann R, et al. Unrelated donor stem cell transplantation compared with chemotherapy for children with acute lymphoblastic leukemia in a second remission: a matched-pair analysis. Blood. 2003;101:3835–3839. - PubMed
-
- Eapen M, Raetz E, Zhang MJ, et al. Outcomes after HLA-matched sibling transplantation or chemotherapy in children with B-precursor acute lymphoblastic leukemia in a second remission: a collaborative study of the Children’s Oncology Group and the Center for International Blood and Marrow Transplant Research. Blood. 2006;107:4961–4967. - PMC - PubMed
-
- Bensinger W. Hi-dose preparative regimens. In: Appelbaum F, Forman SJ, Negrin RS, Blume KG, editors. Hematopoietic Cell Transplantation. Wiley-Blackwell Science; Chichester, United Kingdom: 1999. pp. 1316–1332.
-
- Davies SM, Ramsay NK, Klein JP, et al. Comparison of preparative regimens in transplants for children with acute lymphoblastic leukemia. J Clin Oncol. 2000;18:340–347. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
