

A systematic review and meta-analysis of studies comparing laparoscopic and open distal pancreatectomy
- PMID: 23043660
- PMCID: PMC3482667
- DOI: 10.1111/j.1477-2574.2012.00531.x
A systematic review and meta-analysis of studies comparing laparoscopic and open distal pancreatectomy
Abstract
Objectives: Currently, laparoscopic distal pancreatectomy (LDP) is regarded as a safe and effective surgical approach for lesions in the body and tail of the pancreas. This review compares outcomes of the laparoscopic technique with those of open distal pancreatectomy (ODP) and assesses the efficacy, safety and feasibility of each type of procedure.
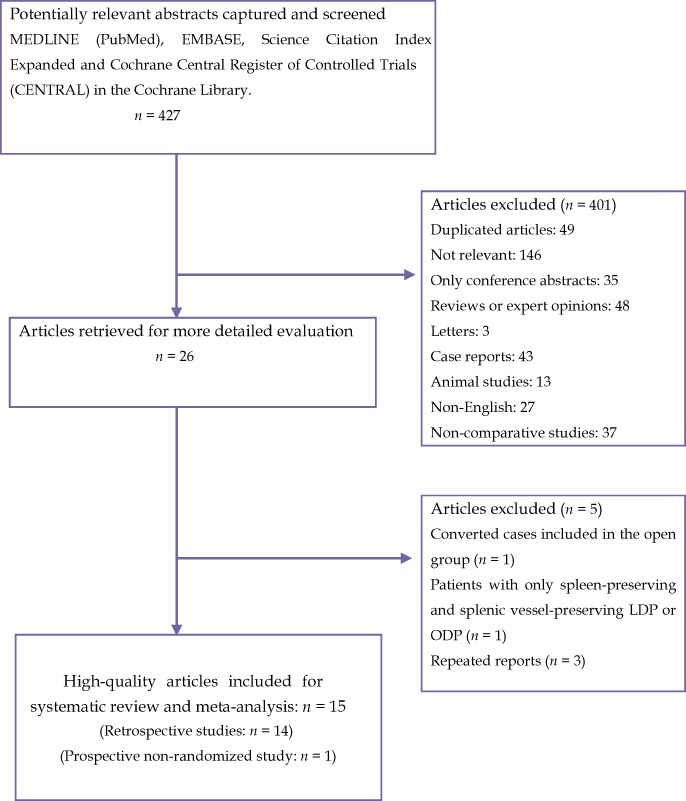
Methods: Comparative studies published between January 1996 and April 2012 were included. Studies were selected based on specific inclusion and exclusion criteria. Evaluated endpoints were operative outcomes, postoperative recovery and postoperative complications.
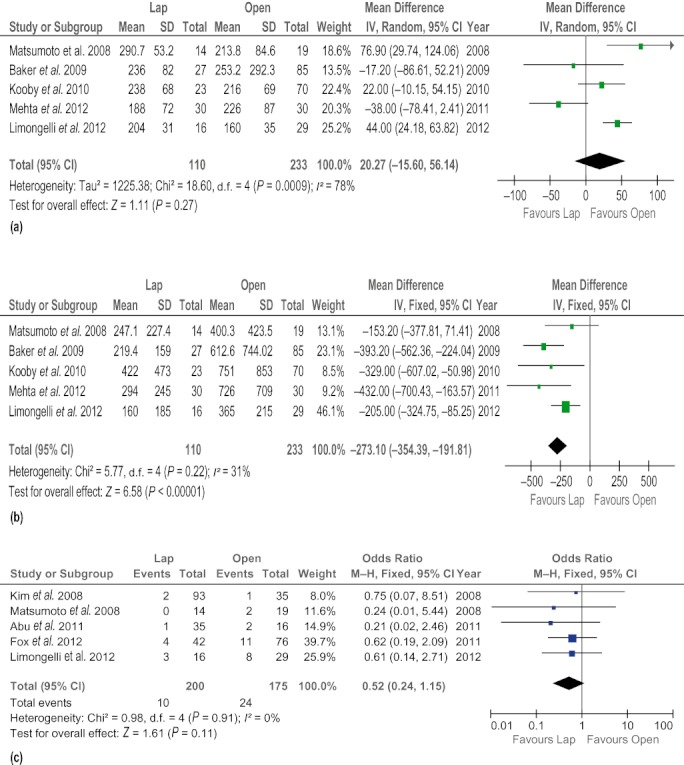
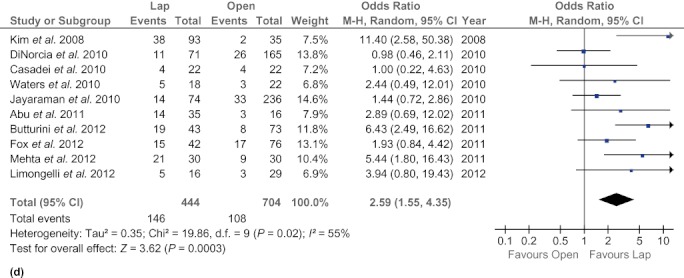
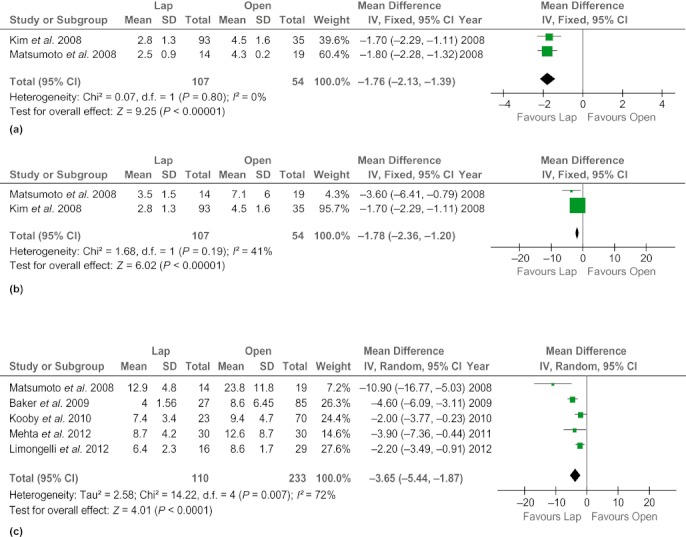
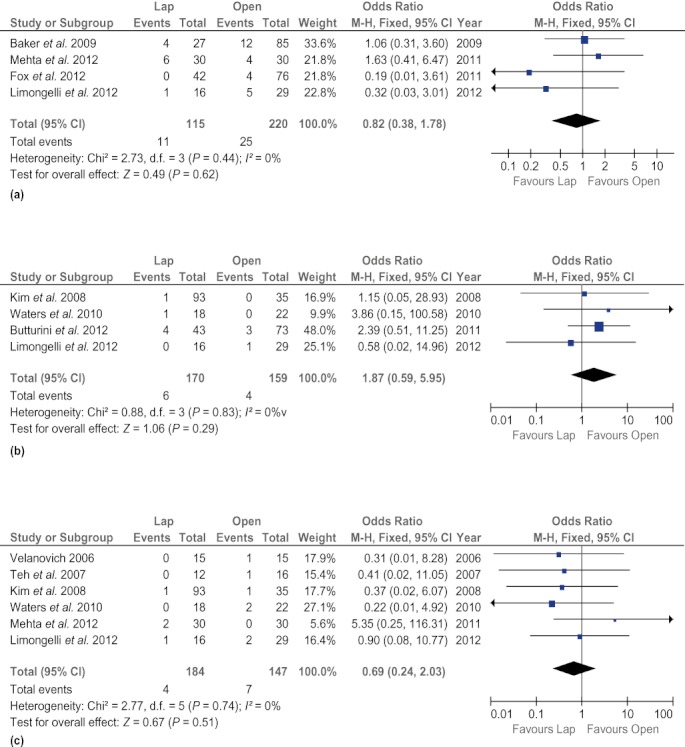
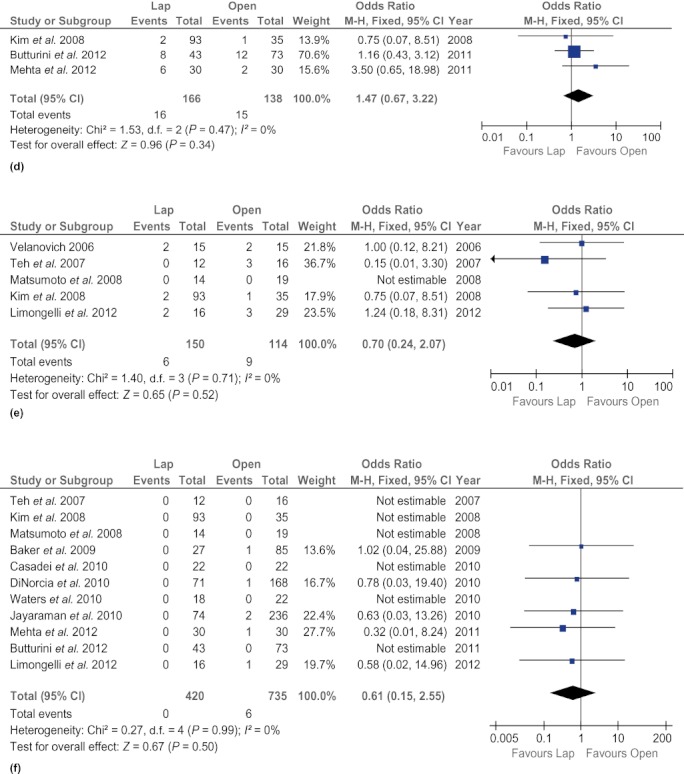
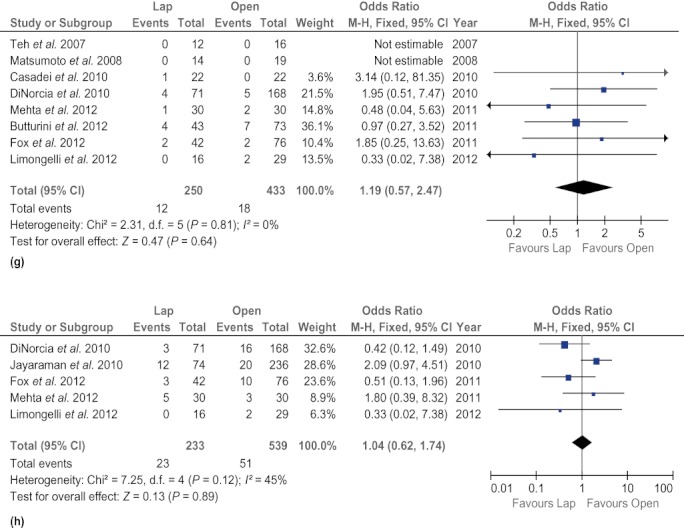
Results: Fifteen non-randomized comparative studies that recruited a total of 1456 patients were analysed. Rates of conversion from LDP to open surgery ranged from 0% to 30%. Patients undergoing LDP had less intraoperative blood loss [weighted mean difference (WMD) -263.36.59 ml, 95% confidence interval (CI) -330.48 to -196.23 ml], fewer blood transfusions [odds ratio (OR) 0.28, 95% CI 0.11-0.76], shorter hospital stay (WMD -4.98 days, 95% CI -7.04 to -2.92 days), a higher rate of splenic preservation (OR 2.98, 95% CI 2.18-3.91), earlier oral intake (WMD -2.63 days, 95% CI -4.23 to 1.03 days) and fewer surgical site infections (OR 0.37, 95% CI 0.18-0.75). However, there were no differences between the two approaches with regard to operation time, time to first flatus and the occurrence of pancreatic fistula and other postoperative complications.
Conclusions: Laparoscopic resection results in improved operative and postoperative outcomes compared with open surgery according to the results of the present meta-analyses. It may be a safe and feasible option for patients with lesions in the body and tail of the pancreas. However, randomized controlled trials should be undertaken to confirm the relevance of these early findings.
© 2012 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Smith CD, Weber CJ, Amerson JR. Laparoscopic adrenalectomy: new gold standard. World J Surg. 1999;23:389–396. - PubMed
-
- Song KB, Kim SC, Park JB, Kim YH, Jung YS, Kim MH, et al. Single-centre experience of laparoscopic left pancreatic resection in 359 consecutive patients: changing the surgical paradigm of left pancreatic resection. Surg Endosc. 2011;25:3364–3372. - PubMed
-
- Velanovich V. Case–control comparison of laparoscopic versus open distal pancreatectomy. J Gastrointest Surg. 2006;10:95–98. - PubMed
-
- Teh SH, Tseng D, Sheppard BC. Laparoscopic and open distal pancreatic resection for benign pancreatic disease. J Gastrointest Surg. 2007;11:1120–1125. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
