

Obesity and risk of recurrence or death after adjuvant endocrine therapy with letrozole or tamoxifen in the breast international group 1-98 trial
- PMID: 23045588
- PMCID: PMC3488270
- DOI: 10.1200/JCO.2011.40.8666
Obesity and risk of recurrence or death after adjuvant endocrine therapy with letrozole or tamoxifen in the breast international group 1-98 trial
Abstract
Purpose: To examine the association of baseline body mass index (BMI) with the risk of recurrence or death in postmenopausal women with early-stage breast cancer receiving adjuvant tamoxifen or letrozole in the Breast International Group (BIG) 1-98 trial at 8.7 years of median follow-up.
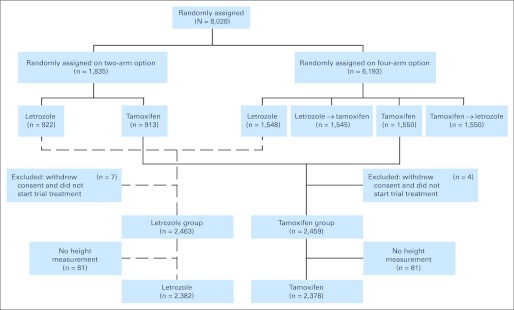
Patients and methods: This report analyzes 4,760 patients with breast cancer randomly assigned to 5 years of monotherapy with letrozole or tamoxifen in the BIG 1-98 trial with available information on BMI at randomization. Multivariable Cox modeling assessed the association of BMI with disease-free survival, overall survival (OS), breast cancer-free interval, and distant recurrence-free interval and tested for treatment-by-BMI interaction. Median follow-up was 8.7 years.
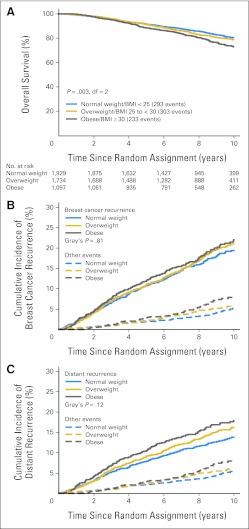
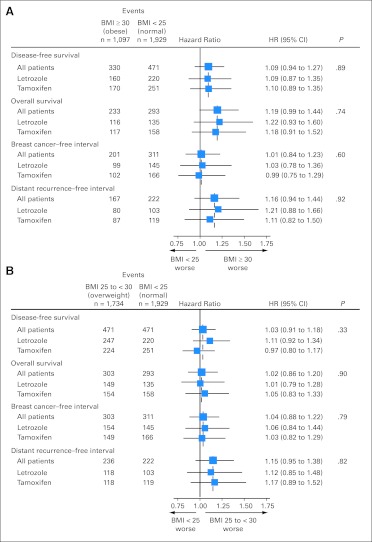
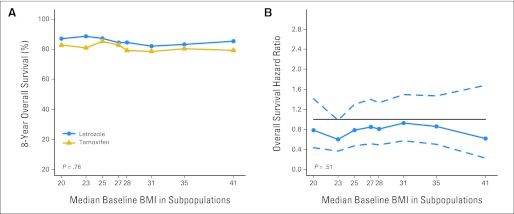
Results: Seventeen percent of patients have died. Obese patients (BMI ≥ 30 kg/m(2)) had slightly poorer OS (hazard ratio [HR] = 1.19; 95% CI, 0.99 to 1.44) than patients with normal BMI (< 25 kg/m(2)), whereas no trend in OS was observed in overweight (BMI 25 to < 30 kg/m(2)) versus normal-weight patients (HR = 1.02; 95% CI, 0.86 to 1.20). Treatment-by-BMI interactions were not statistically significant. The HRs for OS comparing obese versus normal BMI were HR = 1.22 (95% CI, 0.93 to 1.60) and HR = 1.18 (95% CI, 0.91 to 1.52) in the letrozole and tamoxifen groups, respectively.
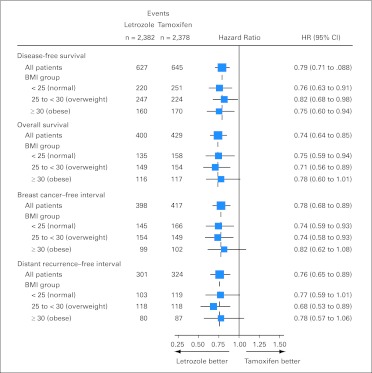
Conclusion: There was no evidence that the benefit of letrozole over tamoxifen differed according to patients' BMI.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Protani M, Coory M, Martin JH. Effect of obesity on survival of women with breast cancer: Systematic review and meta-analysis. Breast Cancer Res Treat . 2010;123:627–635. - PubMed
-
- Ewertz M, Jensen MB, Gunnarsdóttir KÁ, et al. Effect of obesity on prognosis after early-stage breast cancer. J Clin Oncol . 2011;29:25–31. - PubMed
-
- Chlebowski RT, Aiello E, McTiernan A. Weight loss in breast cancer patient management. J Clin Oncol . 2002;20:1128–1143. - PubMed
-
- Rose DP, Vona-Davis L. Influence of obesity on breast cancer receptor status and prognosis. Expert Rev Anticancer Ther . 2009;9:1091–1101. - PubMed
-
- Griggs JJ, Sorbero ME, Lyman GH. Undertreatment of obese women receiving breast cancer chemotherapy. Arch Intern Med . 2005;165:1267–1273. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
