

Syndromic insulin resistance: models for the therapeutic basis of the metabolic syndrome and other targets of insulin resistance
- PMID: 23047930
- PMCID: PMC3875336
- DOI: 10.4158/EP12139.RA
Syndromic insulin resistance: models for the therapeutic basis of the metabolic syndrome and other targets of insulin resistance
Abstract
Objective: To investigate the link between insulin resistance and the metabolic syndrome how to develop treatment approaches.
Methods: We present 3 cases of extreme syndromic insulin resistance: lipodystrophy, autoantibodies to the insulin receptor, and mutations in the insulin receptor gene, with accompanying discussion of pathophysiology and treatment.
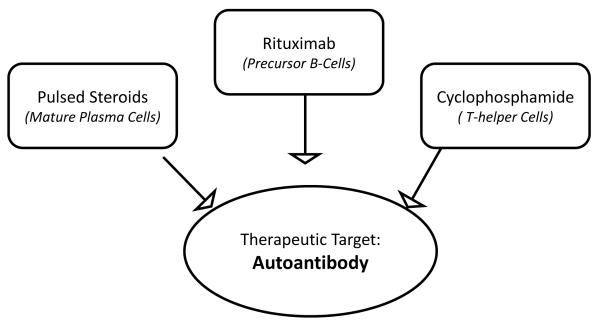
Results: In lipodystrophy, insulin resistance is a direct consequence of leptin deficiency, and thus leptin replacement reverses metabolic syndrome abnormalities, including diabetes and hypertriglyceridemia. The insulin "receptoropathies," including autoantibodies to the insulin receptor and insulin receptor gene mutations, are characterized by extreme insulin resistance and ovarian hyperandrogenism, without dyslipidemia or fatty liver disease. Autoantibodies to the insulin receptor can be treated using an immunosuppressive paradigm adapted from treatment of other autoimmune and neoplastic conditions. Leptin treatment has shown some success in treating hyperglycemia in patients with insulin receptor gene mutations. Treatment for this condition remains inadequate, and novel therapies that bypass insulin receptor signaling, such as enhancers of brown adipose tissue, are needed.
Conclusions: We present a clinical approach to the treatment of syndromic insulin resistance. The study of rare diseases that replicate the metabolic syndrome, with clear-cut pathophysiology, promotes understanding of novel physiology and development of targeted therapies that may be applicable to the broader population with obesity, insulin resistance, and diabetes.
Figures

References
-
- Must A, Spadano J, Coakley EH, Field AE, Colditz G, Dietz WH. The Disease Burden Associated With Overweight and Obesity. JAMA. 1999;282:1523–1529. - PubMed
-
- Bray GA. Medical consequences of obesity. J Clin Endocrinol Metab. 2004;89:2583–2589. - PubMed
-
- Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity in the United States, 2009-2010. National Center for Health Statistics; Hyattsville, MD: 2012. NCHS data brief, no 82.
-
- Centers for Disease Control and Prevention . National diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States, 2011. Department of Health and Human Services, Centers for Disease Control and Prevention; Atlanta, GA: 2011.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
