

Tocolytic therapy for preterm delivery: systematic review and network meta-analysis
- PMID: 23048010
- PMCID: PMC4688428
- DOI: 10.1136/bmj.e6226
Tocolytic therapy for preterm delivery: systematic review and network meta-analysis
Abstract
Objective: To determine the most effective tocolytic agent at delaying delivery.
Design: Systematic review and network meta-analysis.
Data sources: Cochrane Central Register of Controlled Trials, Medline, Medline In-Process, Embase, and CINAHL up to 17 February 2012.
Study selection: Randomised controlled trials of tocolytic therapy in women at risk of preterm delivery.
Data extraction: At least two reviewers extracted data on study design, characteristics, number of participants, and outcomes reported (neonatal and maternal). A network meta-analysis was done using a random effects model with drug class effect. Two sensitivity analyses were carried out for the primary outcome; restricted to studies at low risk of bias and restricted to studies excluding women at high risk of preterm delivery (those with multiple gestation and ruptured membranes).
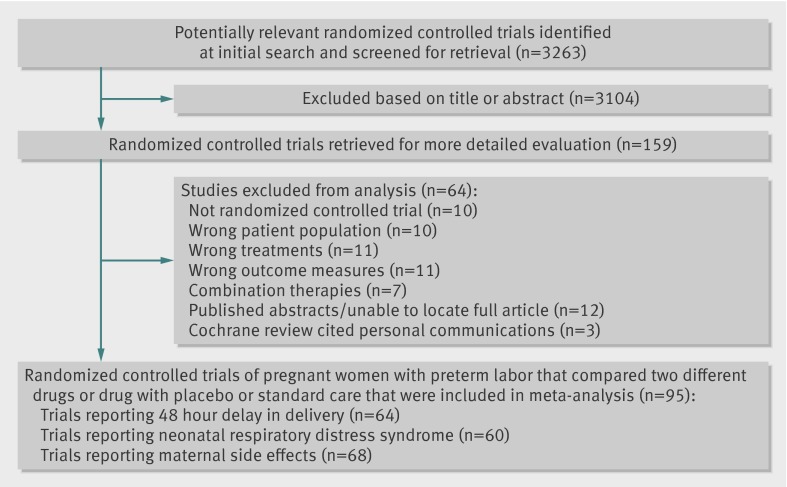
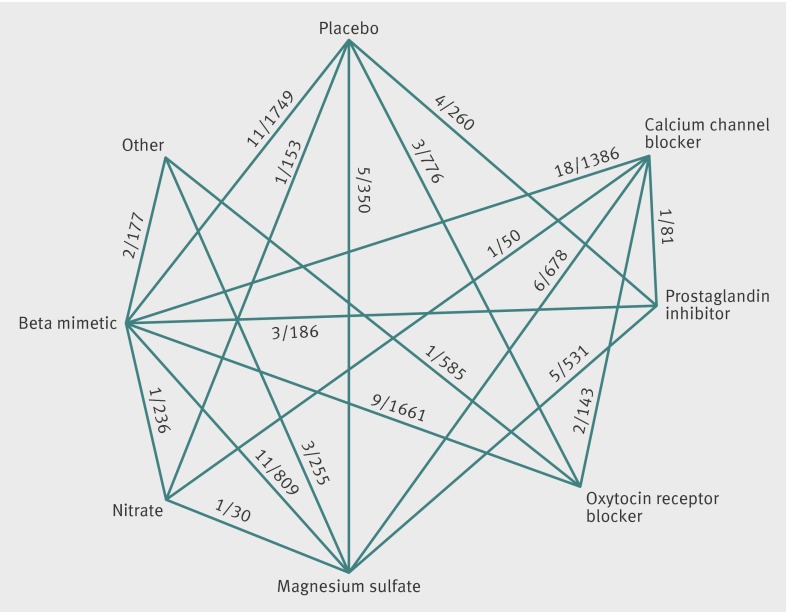
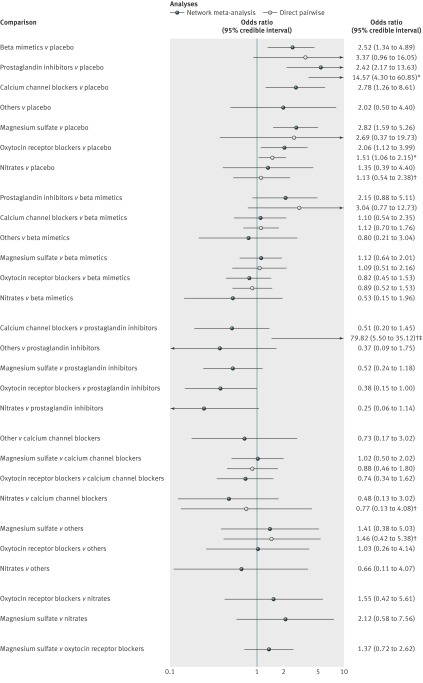
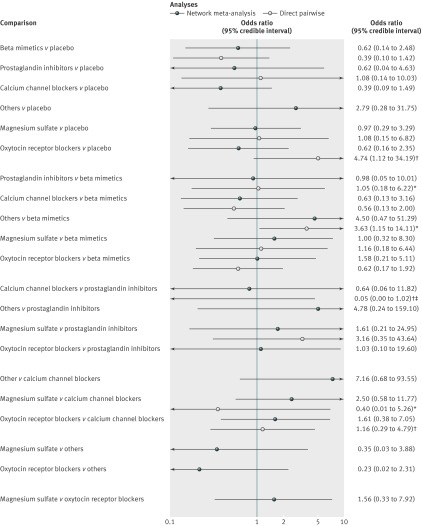
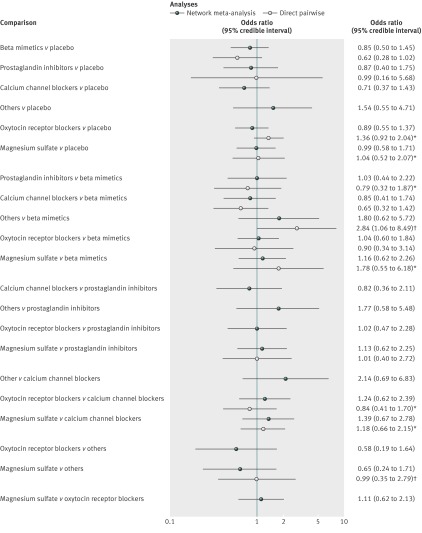
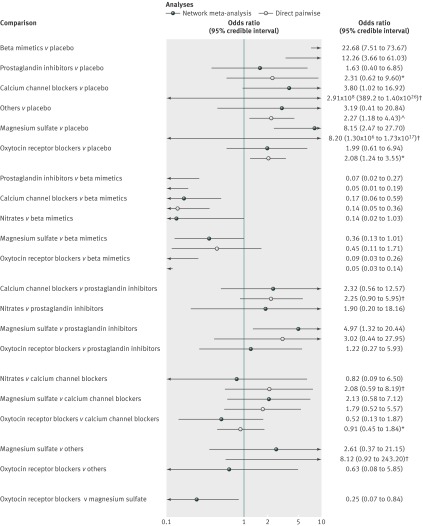
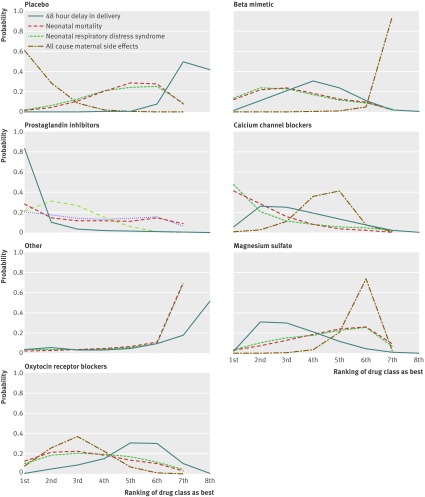
Results: Of the 3263 titles initially identified, 95 randomized controlled trials of tocolytic therapy were reviewed. Compared with placebo, the probability of delivery being delayed by 48 hours was highest with prostaglandin inhibitors (odds ratio 5.39, 95% credible interval 2.14 to 12.34) followed by magnesium sulfate (2.76, 1.58 to 4.94), calcium channel blockers (2.71, 1.17 to 5.91), beta mimetics (2.41, 1.27 to 4.55), and the oxytocin receptor blocker atosiban (2.02, 1.10 to 3.80). No class of tocolytic was significantly superior to placebo in reducing neonatal respiratory distress syndrome. Compared with placebo, side effects requiring a change of medication were significantly higher for beta mimetics (22.68, 7.51 to 73.67), magnesium sulfate (8.15, 2.47 to 27.70), and calcium channel blockers (3.80, 1.02 to 16.92). Prostaglandin inhibitors and calcium channel blockers were the tocolytics with the best probability of being ranked in the top three medication classes for the outcomes of 48 hour delay in delivery, respiratory distress syndrome, neonatal mortality, and maternal side effects (all cause).
Conclusions: Prostaglandin inhibitors and calcium channel blockers had the highest probability of delaying delivery and improving neonatal and maternal outcomes.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Tocolytics: do they actually work?BMJ. 2012 Oct 9;345:e6531. doi: 10.1136/bmj.e6531. BMJ. 2012. PMID: 23048012 No abstract available.
-
Network meta-analysis shows that prostaglandin inhibitors and nifedipine are best short-term tocolytics for preterm delivery.Evid Based Med. 2013 Oct;18(5):182-3. doi: 10.1136/eb-2012-101128. Epub 2013 Feb 5. Evid Based Med. 2013. PMID: 23386705 No abstract available.
References
-
- Haas DM, Imperiale TF, Kirkpatrick PR, Klein RW, Zollinger TW, Golichowski AM. Tocolytic therapy: a meta-analysis and decision analysis. Obset Gynecol 2009;113:585-94. - PubMed
-
- Roberts D, Dalziel SR. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev 2006;(3):CD004454. - PubMed
-
- Hamilton BE, Martin JA, Ventura SJ. Births: preliminary data for 2008. Natl Vital Stat Rep 2010;58:1-17. - PubMed
-
- ACOG practice bulletin. Management of preterm labor. No 43, May 2003. Obstet Gynecol 2003;101:1039-47. - PubMed
-
- Goldenberg RL. The management of preterm labor. Obstet Gynecol 2002;100:1020-37. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical