

Pulmonary metastasectomy for sarcoma: a systematic review of reported outcomes in the context of Thames Cancer Registry data
- PMID: 23048062
- PMCID: PMC3488730
- DOI: 10.1136/bmjopen-2012-001736
Pulmonary metastasectomy for sarcoma: a systematic review of reported outcomes in the context of Thames Cancer Registry data
Abstract
Objectives: Sarcoma has a predilection to metastasis to the lungs. Surgical excision of these metastases (pulmonary metastasectomy) when possible has become standard practice. We reviewed the published selection and outcome data.
Design: Systematic review of published reports that include survival rates or any other outcome data. Survival data were put in the context of those in a cancer registry.
Setting: Specialist thoracic surgical centres reporting the selection and outcome for pulmonary metastasectomy in 18 follow-up studies published 1991-2010.
Participants: Patients having one or more of 1357 pulmonary metastasectomy operations performed between 1980 and 2006.
Interventions: All patients had surgical pulmonary metastasectomy. A first operation was reported in 1196 patients. Of 1357 patients, 43% had subsequent metastasectomy, some having 10 or more thoracotomies. Three studies were confined to patients having repeated pulmonary metastasectomy.
Primary and secondary outcome measures: Survival data to various time points usually 5 years and sometimes 3 or 10 years. No symptomatic or quality of life data were reported.
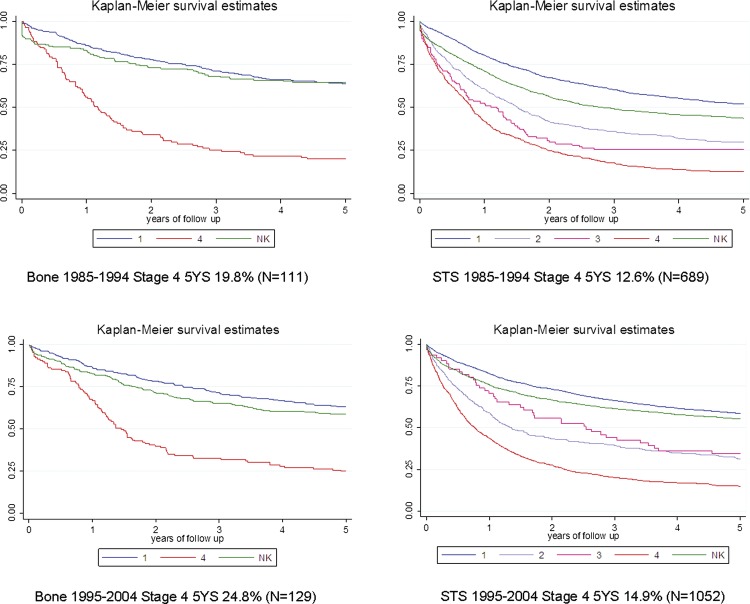
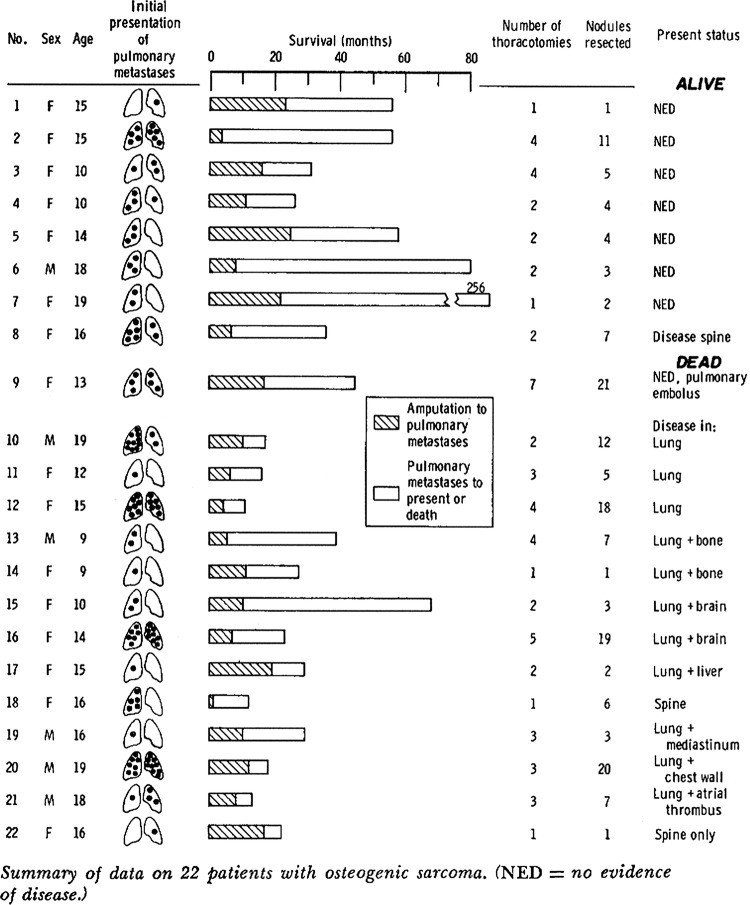
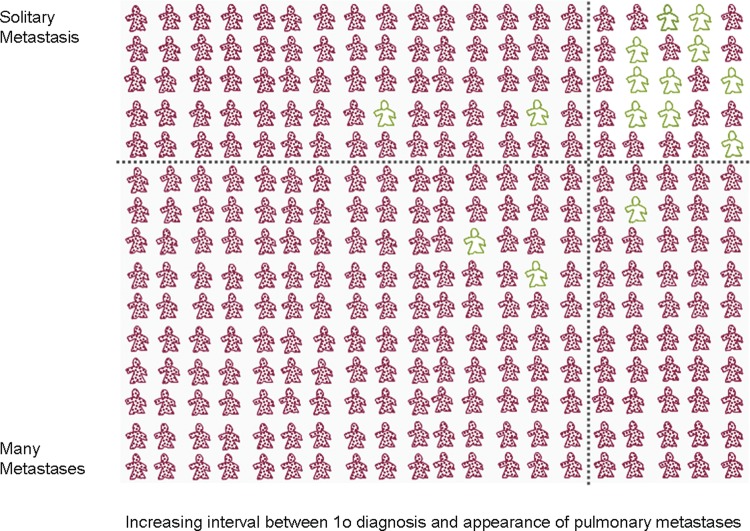
Results: About 34% and 25% of patients were alive 5 years after a first metastasectomy operation for bone or soft tissues sarcoma respectively. Better survival was reported with fewer metastases and longer intervals between diagnosis and the appearance of metastases. In the Thames Cancer Registry for 1985-1994 and 1995-2004 5 year survival rates for all patients with metastatic sarcoma were 20% and 25% for bone, and for soft tissue sarcoma 13% and 15%.
Conclusions: The 5 year survival rate among sarcoma patients who are selected to have pulmonary metastasectomy is higher than that observed among unselected registry data for patients with any metastatic disease at diagnosis. There is no evidence that survival difference is attributable to metastasectomy. No data were found on respiratory or any other symptomatic benefit. Given the certain harm associated with thoracotomy, often repeated, better evidence is required.
Figures
References
-
- Kager L, Zoubek A, Potschger U, et al. Primary metastatic osteosarcoma: presentation and outcome of patients treated on neoadjuvant Cooperative Osteosarcoma Study Group protocols. J Clin Oncol 2003;21:2011–18 - PubMed
-
- Gelderblom H, Jinks RC, Sydes M, et al. Survival after recurrent osteosarcoma: data from 3 European Osteosarcoma Intergroup (EOI) randomized controlled trials. Eur J Cancer 2011;47:895–902 - PubMed
-
- National Institute for Health and Clinical Excellence (NICE) Guidance on cancer services. Improving outcomes for people with sarcoma. The manual. The National Institute for Health and Clinical Excellence (NICE) 2006. http://www.nice.org.uk/nicemedia/live/10903/28934/28934.pdf (accessed 21 Sep 2012).
-
- National Institute of Health and Clinical Excellence (NICE) Guidance on cancer services. Improving outcomes for people with sarcoma. The evidence review. Institute of Health and Clinical Excellence, 2006. http://www.nice.org.uk/nicemedia/live/10903/28936/28936.pdf (accessed 21 Sep 2012).
-
- Whooley BP, Gibbs JF, Mooney MM, et al. Primary extremity sarcoma: what is the appropriate follow-up? Ann Surg Oncol 2000;7:9–14 - PubMed
LinkOut - more resources
Full Text Sources
Medical