

Diagnostic and therapeutic challenges of intracranial hemorrhage in neonates with congenital hemophilia: a case report and review
- PMID: 23049462
- PMCID: PMC3448247
Diagnostic and therapeutic challenges of intracranial hemorrhage in neonates with congenital hemophilia: a case report and review
Abstract
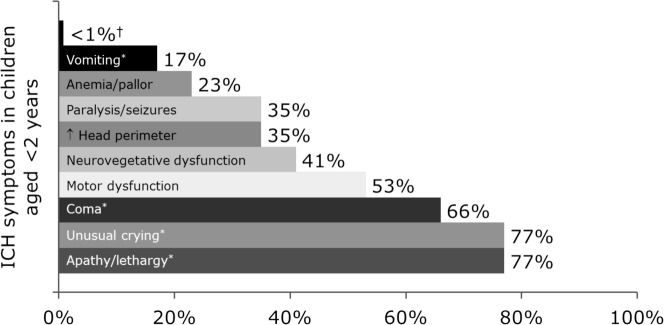
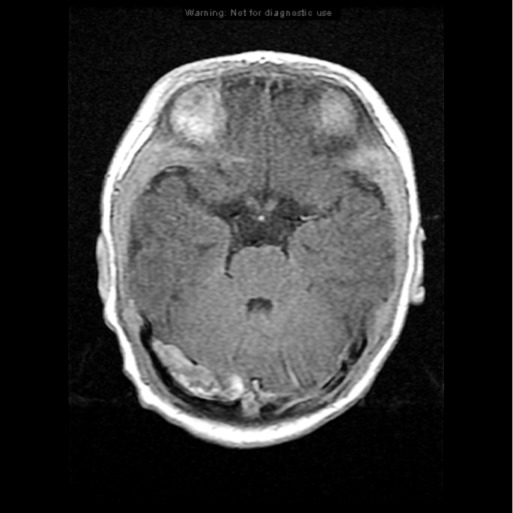
Intracranial hemorrhage (ICH) in full-term neonates with hemophilia is uncommon. Retrospective studies estimate the incidence to be 3.4%-4.0%. However, ICH is the second most common initial hemorrhage for all infants with congenital hemophilia. Nearly half (41%) of the hemorrhages occur within the first week of life, and most hemorrhages are related to traumatic deliveries. But clinical signs of ICH in neonates are difficult to assess and often result in a delay in the diagnosis. The timely diagnosis of ICH is critical; however, the early and intensive factor replacement therapy that the patient needs is associated with the risk of inhibitor formation. We report a case of ICH in a neonate with severe hemophilia A, no family history, and inhibitor development after intensive therapy.
Keywords: Hemophilia; intracranial hemorrhage; neonatology.
Conflict of interest statement
Figures
Similar articles
-
Hemophilia A presenting with intracranial hemorrhage in neonate: a case report.Zhonghua Yi Xue Za Zhi (Taipei). 1994 Jul;54(1):62-6. Zhonghua Yi Xue Za Zhi (Taipei). 1994. PMID: 8087725
-
Neonatal hemophilia B with intracranial hemorrhage. Case report.Am J Pediatr Hematol Oncol. 1988 Fall;10(3):244-8. doi: 10.1097/00043426-198823000-00012. Am J Pediatr Hematol Oncol. 1988. PMID: 3052146 Review.
-
Incidence and mortality rates of intracranial hemorrhage in hemophilia: a systematic review and meta-analysis.Blood. 2021 Dec 30;138(26):2853-2873. doi: 10.1182/blood.2021011849. Blood. 2021. PMID: 34411236
-
Intracranial hemorrhage in congenital bleeding disorders.Blood Coagul Fibrinolysis. 2018 Jan;29(1):1-11. doi: 10.1097/MBC.0000000000000660. Blood Coagul Fibrinolysis. 2018. PMID: 28901996 Review.
-
A Retrospective Analysis of Intracranial Hemorrhage in Children with Hemophilia A.Curr Med Sci. 2018 Oct;38(5):875-879. doi: 10.1007/s11596-018-1956-4. Epub 2018 Oct 20. Curr Med Sci. 2018. PMID: 30341523
Cited by
-
ACTH therapy for West syndrome with severe hemophilia A.Epilepsy Behav Case Rep. 2016 May 10;6:1-2. doi: 10.1016/j.ebcr.2016.04.007. eCollection 2016. Epilepsy Behav Case Rep. 2016. PMID: 27896066 Free PMC article.
-
Intracranial haemorrhage in children and adults with haemophilia A and B: a literature review of the last 20 years.Blood Transfus. 2019 Sep;17(5):378-384. doi: 10.2450/2019.0253-18. Epub 2018 Feb 4. Blood Transfus. 2019. PMID: 30747705 Free PMC article. Review.
-
Acute Life-Threatening Hemorrhage in Neonates With Severe Hemophilia A: A Report of 3 Cases.J Investig Med High Impact Case Rep. 2018 Sep 18;6:2324709618800349. doi: 10.1177/2324709618800349. eCollection 2018 Jan-Dec. J Investig Med High Impact Case Rep. 2018. PMID: 30246038 Free PMC article.
-
Outcome and Predisposing Factors for Intracranial Hemorrhage in Turkish Children with Hemophilia.J Clin Med. 2025 Jan 22;14(3):689. doi: 10.3390/jcm14030689. J Clin Med. 2025. PMID: 39941359 Free PMC article.
-
Emicizumab prophylaxis in infants with hemophilia A (HAVEN 7): primary analysis of a phase 3b open-label trial.Blood. 2024 Apr 4;143(14):1355-1364. doi: 10.1182/blood.2023021832. Blood. 2024. PMID: 38127586 Free PMC article. Clinical Trial.
References
-
- Ljung R, Lindgren AC, Petrini P, Tengborn L. Normal vaginal delivery is to be recommended for haemophilia carrier gravidae. Acta Paediatr. 1994 Jun;83(6):609–611. - PubMed
-
- Kulkarni R, Lusher JM. Intracranial and extracranial hemorrhages in newborns with hemophilia: a review of the literature. J Pediatr Hematol Oncol. 1999 Jul-Aug;21(4):289–295. - PubMed
-
- Kulkarni R, Soucie JM, Lusher J, et al. Haemophilia Treatment Center Network Investigators. Sites of initial bleeding episodes, mode of delivery and age of diagnosis in babies with haemophilia diagnosed before the age of 2 years: a report from The Centers for Disease Control and Prevention's (CDC) Universal Data Collection (UDC) project. Haemophilia. 2009 Nov;15(6):1281–1290. Epub 2009 Jul 22. - PubMed
-
- National Hemophilia Foundation. MASAC guidelines for perinatal management of women with bleeding disorders and carriers of hemophilia A and B. MASAC Document 192. 2012. http://hemophilia.org/NHFWeb/Resource/StaticPages/menu0/menu5/menu57/mas.... Accessed January 17.
-
- Myles LM, Massicotte P, Drake J. Intracranial hemorrhage in neonates with unrecognized hemophilia A: a persisting problem. Pediatr Neurosurg. 2001 Feb;34(2):94–97. - PubMed
Publication types
LinkOut - more resources
Full Text Sources