

Hepatitis B virus infection in human immunodeficiency virus infected southern African adults: occult or overt--that is the question
- PMID: 23049685
- PMCID: PMC3462206
- DOI: 10.1371/journal.pone.0045750
Hepatitis B virus infection in human immunodeficiency virus infected southern African adults: occult or overt--that is the question
Abstract
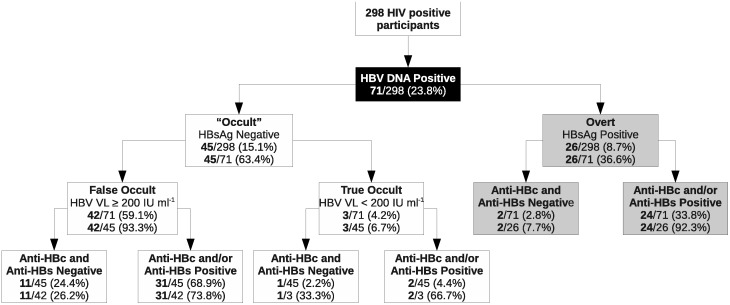
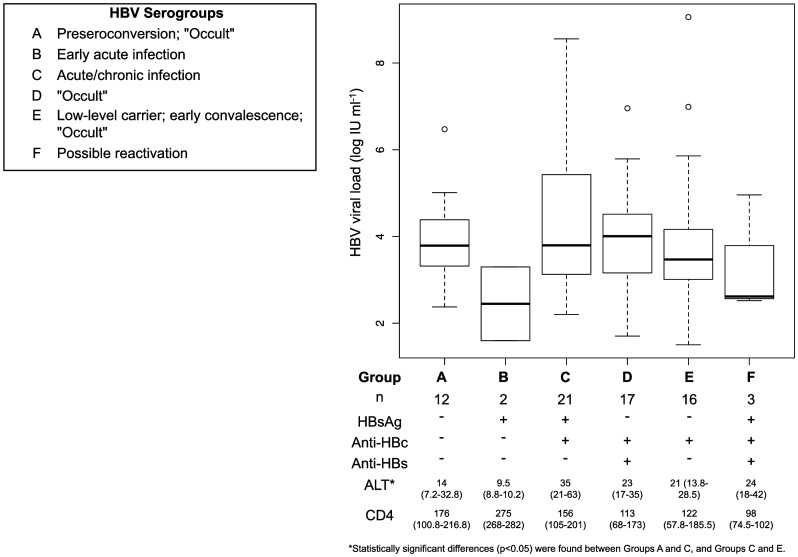
Hepatitis B virus (HBV) and human immunodeficiency virus (HIV) share transmission routes and are endemic in sub-Saharan Africa. The objective of the present study was to use the Taormina definition of occult HBV infection, together with stringent amplification conditions, to determine the prevalence and characteristics of HBV infection in antiretroviral treatment (ART)-naïve HIV(+ve) adults in a rural cohort in South Africa. The presence of HBV serological markers was determined by enzyme linked immunoassay (ELISA) tests. HBV DNA-positivity was determined by polymerase chain reaction (PCR) of at least two of three different regions of the HBV genome. HBV viral loads were determined by real-time PCR. Liver fibrosis was determined using the aspartate aminotransferase-to-platelet ratio index. Of the 298 participants, 231 (77.5%) showed at least one HBV marker, with 53.7% HBV DNA(-ve) (resolved) and 23.8% HBV DNA(+ve) (current) [8.7% HBsAg(+ve): 15.1% HBsAg(-ve)]. Only the total number of sexual partners distinguished HBV DNA(+ve) and HBV DNA(-ve) participants, implicating sexual transmission of HBV and/or HIV. It is plausible that sexual transmission of HBV and/or HIV may result in a new HBV infection, superinfection and re-activation as a consequence of immunesuppression. Three HBsAg(-ve) HBV DNA(+ve) participants had HBV viral loads <200 IU/ml and were therefore true occult HBV infections. The majority of HBsAg(-ve) HBV DNA(+ve) participants did not differ from HBsAg(+ve) HBV DNA(+ve) (overt) participants in terms of HBV viral loads, ALT levels or frequency of liver fibrosis. Close to a quarter of HIV(+ve) participants were HBV DNA(+ve), of which the majority were HBsAg(-ve) and were only detected using nucleic acid testing. Detection of HBsAg(-ve) HBV DNA(+ve) subjects is advisable considering they were clinically indistinguishable from HBsAg(+ve) HBV DNA(+ve) individuals and should not be overlooked, especially if lamivudine is included in the ART.
Conflict of interest statement
Figures
References
-
- UNAIDS (2010) UNAIDS report on the global AIDS epidemic 2010. Available: http://www.unaids.org/en/dataanalysis/. Accessed 2011 November 16.
-
- Kramvis A, Kew MC (2007) Epidemiology of hepatitis B virus in Africa, its genotypes and clinical associations of genotypes. Hepatol Res 37: S9–S19. - PubMed
-
- Burnett RJ, Francois G, Kew MC, Leroux-Roels G, Meheus A, et al. (2005) Hepatitis B virus and human immunodeficiency virus co-infection in sub-Saharan Africa: a call for further investigation. Liver Int 25: 201–213. - PubMed
-
- Chung RT (2006) Hepatitis C and B viruses: the new opportunists in HIV infection. Top HIV Med 14: 78–83. - PubMed
-
- Thio CL, Seaberg EC, Skolasky R, Phair J, Visscher B, et al. (2002) HIV-1, hepatitis B virus, and risk of liver-related mortality in the Multicenter Cohort Study (MACS). Lancet 360: 1921–1926. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
