

Improving the extent of malignant glioma resection by dual intraoperative visualization approach
- PMID: 23049761
- PMCID: PMC3458892
- DOI: 10.1371/journal.pone.0044885
Improving the extent of malignant glioma resection by dual intraoperative visualization approach
Abstract
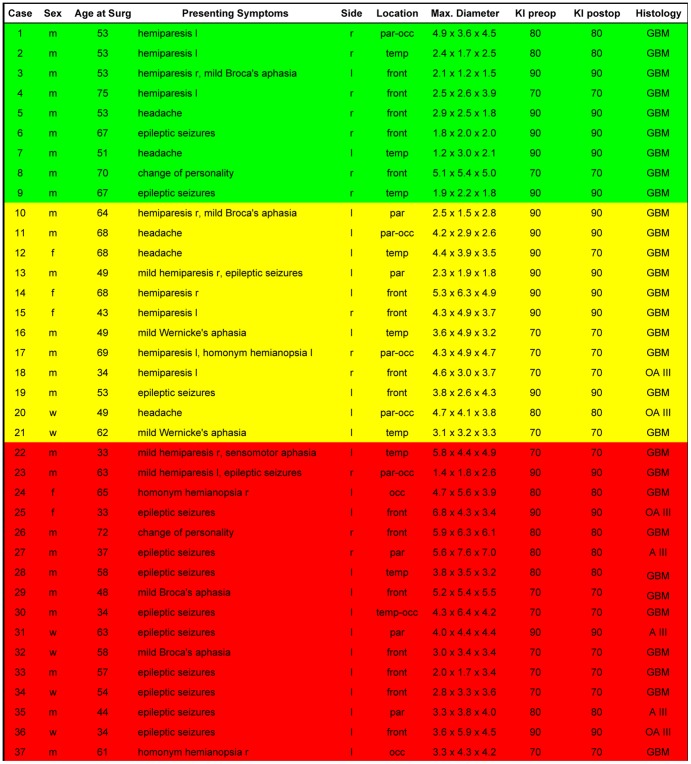
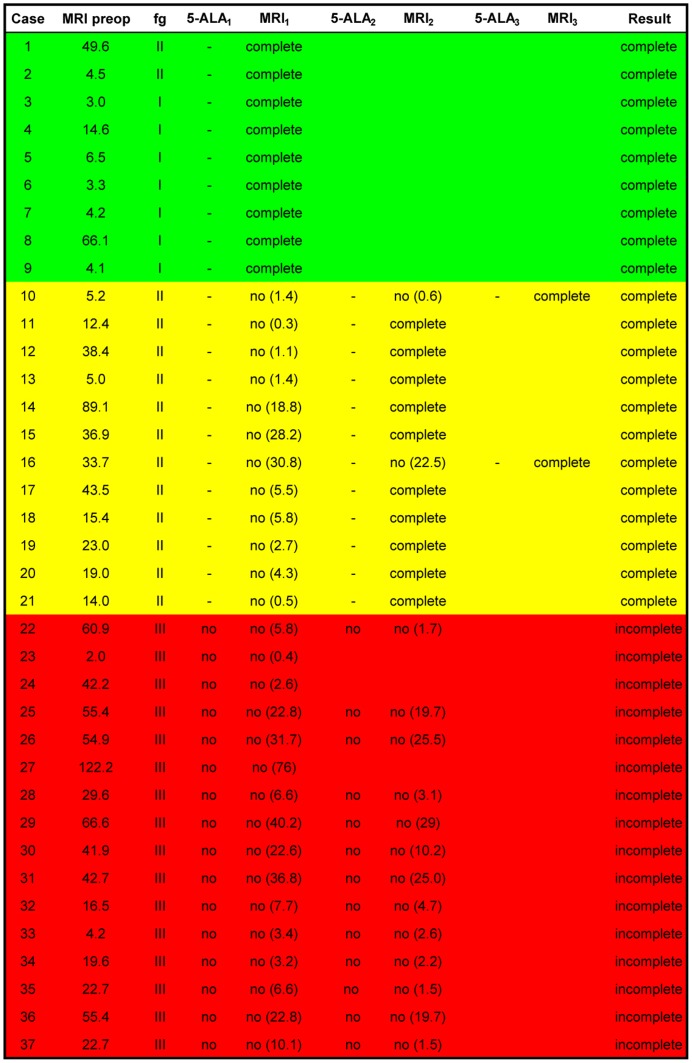
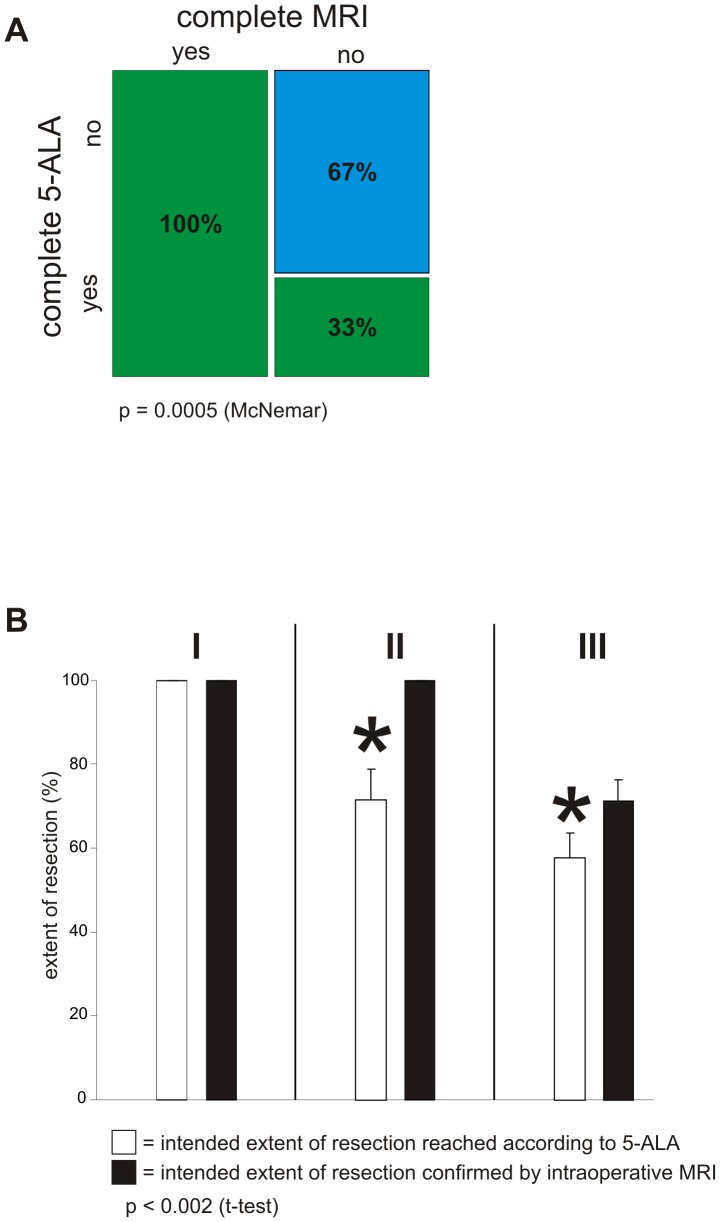
Despite continuing debates around cytoreductive surgery in malignant gliomas, there is broad consensus that increased extent of tumor reduction improves overall survival. However, maximization of the extent of tumor resection is hampered by difficulty in intraoperative discrimination between normal and pathological tissue. In this context, two established methods for tumor visualization, fluorescence guided surgery with 5-ALA and intraoperative MRI (iMRI) with integrated functional neuronavigation were investigated as a dual intraoperative visualization (DIV) approach. Thirty seven patients presumably suffering from malignant gliomas (WHO grade III or IV) according to radiological appearance were included. Twenty-one experimental sequences showing complete resection according to the 5-ALA technique were confirmed by iMRI. Fourteen sequences showing complete resection according to the 5-ALA technique could not be confirmed by iMRI, which detected residual tumor. Further analysis revealed that these sequences could be classified as functional grade II tumors (adjacent to eloquent brain areas). The combination of fluorescence guided resection and intraoperative evaluation by high field MRI significantly increased the extent of tumor resection in this subgroup of malignant gliomas located adjacent to eloquent areas from 61.7% to 100%; 5-ALA alone proved to be insufficient in attaining gross total resection without the danger of incurring postoperative neurological deterioration. Furthermore, in the case of functional grade III gliomas, iMRI in combination with functional neuronavigation was significantly superior to the 5-ALA resection technique. The extent of resection could be increased from 57.1% to 71.2% without incurring postoperative neurological deficits.
Conflict of interest statement
Figures
References
-
- Wen PY, Kesari S (2008) Malignant gliomas in adults. N Engl J Med 359: 492–507. - PubMed
-
- Kubben PL, ter Meulen KJ, Schijns OE, ter Laak-Poort MP, van Overbeeke JJ, et al. (2011) Intraoperative MRI-guided resection of glioblastoma multiforme: a systematic review. Lancet Oncol 12: 1062–1070. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, et al. (2005) Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352: 987–996. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
