

Improved resistance to ischemia and reperfusion, but impaired protection by ischemic preconditioning in patients with type 1 diabetes mellitus: a pilot study
- PMID: 23051145
- PMCID: PMC3504536
- DOI: 10.1186/1475-2840-11-124
Improved resistance to ischemia and reperfusion, but impaired protection by ischemic preconditioning in patients with type 1 diabetes mellitus: a pilot study
Abstract
Background: In patients with type 1 diabetes mellitus (T1DM), cardiovascular events are more common, and the outcome following a myocardial infarction is worse than in nondiabetic subjects. Ischemic or pharmacological preconditioning are powerful interventions to reduce ischemia reperfusion (IR)-injury. However, animal studies have shown that the presence of T1DM can limit these protective effects. Therefore, we aimed to study the protective effect of ischemic preconditioning in patients with T1DM, and to explore the role of plasma insulin and glucose on this effect.
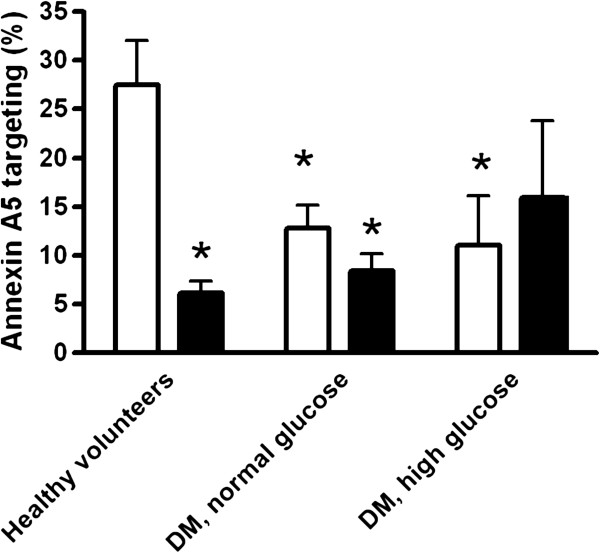
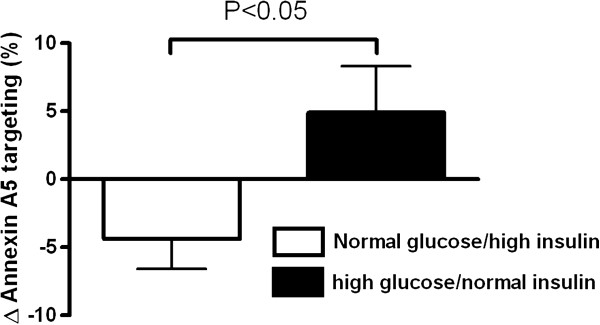
Methods: 99mTechnetium-annexin A5 scintigraphy was used to detect IR-injury. IR-injury was induced by unilateral forearm ischemic exercise. At reperfusion, Tc-annexin A5 was administered, and IR-injury was expressed as the percentage difference in radioactivity in the thenar muscle between the experimental and control arm 4 hours after reperfusion. 15 patients with T1DM were compared to 21 nondiabetic controls. The patients were studied twice, with or without ischemic preconditioning (10 minutes of forearm ischemia and reperfusion). Patients were studied in either normoglycemic hyperinsulinemic conditions (n=8) or during hyperglycemic normoinsulinemia (n=7). The controls were studied once either with (n=8) or without (n=13) ischemic preconditioning.
Results: Patients with diabetes were less vulnerable to IR-injury than nondiabetic healthy controls (12.8 ± 2.4 and 11.0 ± 5.1% versus 27.5 ± 4.5% in controls; p<0.05). The efficacy of ischemic preconditioning to reduce IR-injury, however, was lower in the patients and was even completely abolished during hyperglycemia.
Conclusions: Patients with T1DM are more tolerant to forearm IR than healthy controls in our experimental model. The efficacy of ischemic preconditioning to limit IR-injury, however, is reduced by acute hyperglycemia.
Trial registration: The study is registered at www.clinicaltrials.gov (NCT00184821).
Figures
References
-
- Mathew V, Gersh BJ, Williams BA, Laskey WK, Willerson JT, Tilbury RT, Davis BR, Holmes DR Jr. Outcomes in patients with diabetes mellitus undergoing percutaneous coronary intervention in the current era: a report from the Prevention of REStenosis with Tranilast and its Outcomes (PRESTO) trial. Circulation. 2004;109:476–480. doi: 10.1161/01.CIR.0000109693.64957.20. - DOI - PubMed
-
- van Straten AH, Soliman Hamad MA, van Zundert AA, Martens EJ, Schonberger JP, ter Woorst JF, de Wolf AM. Diabetes and survival after coronary artery bypass grafting: comparison with an age- and sex-matched population. Eur J Cardiothorac Surg. 2010;37:1068–1074. doi: 10.1016/j.ejcts.2009.11.042. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
