

Long-term fecal diverting device for the prevention of sepsis in case of colorectal anastomotic leakage: an animal experiment
- PMID: 23053676
- PMCID: PMC3639361
- DOI: 10.1007/s00384-012-1580-x
Long-term fecal diverting device for the prevention of sepsis in case of colorectal anastomotic leakage: an animal experiment
Abstract
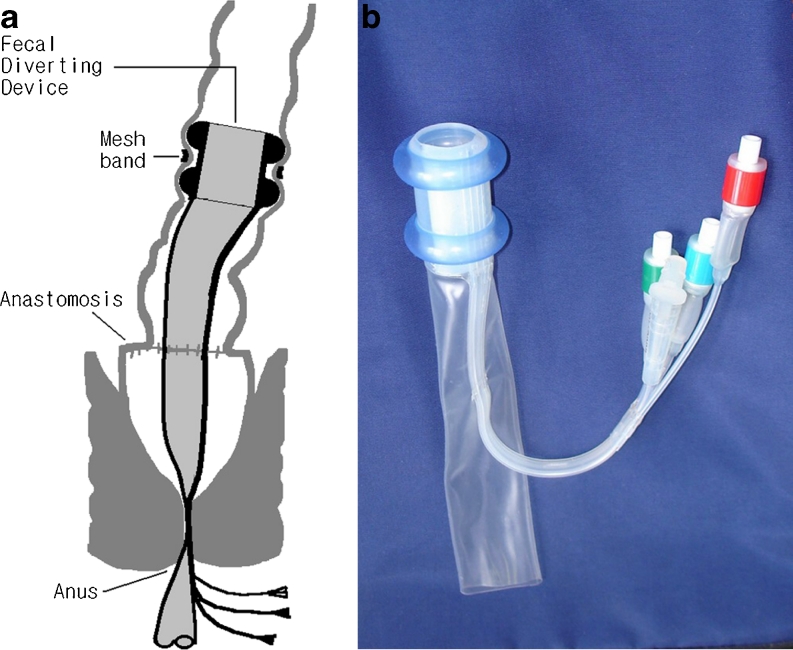
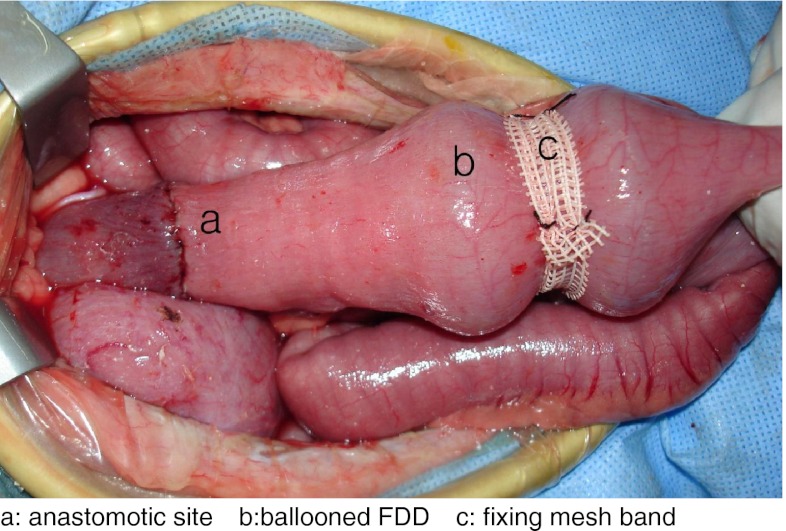
Background: A new fecal diverting device (FDD) was fabricated for fecal diversion from the proximal colon above the anastomosis to outside the anus for protecting the rectal anastomosis. The aim of the study is to evaluate the safety and effectiveness of the FDD.
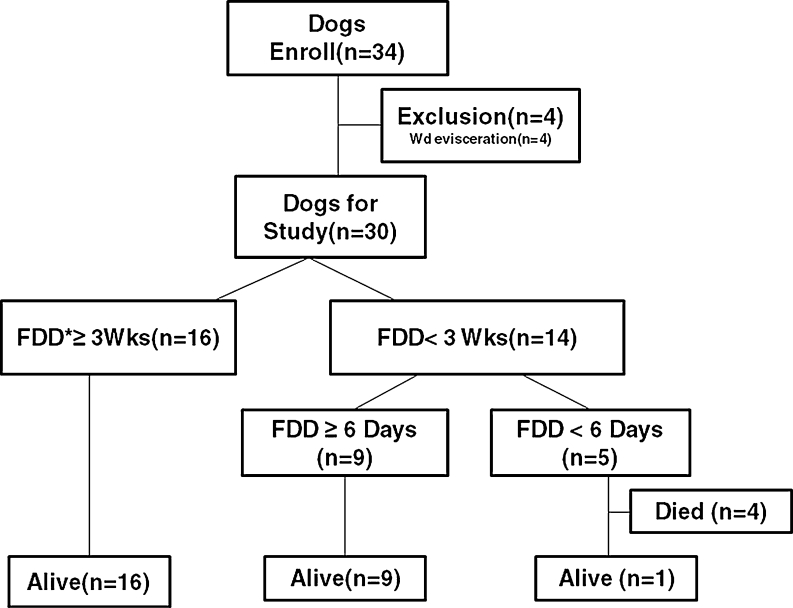
Methods: After a pilot study, a prospective observational trial was performed in 34 mongrel dogs. The experiment comprised of segmental resection and anastomosis of the colon, fixation of the FDD, and observation for 3 weeks (n = 15) and more than 3 weeks (n = 19) without initiation of parenteral nutrition.
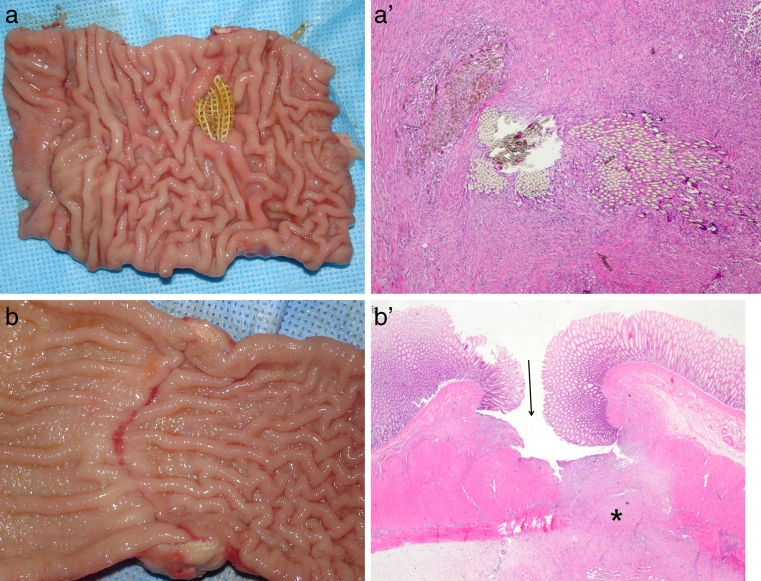
Results: Four cases of perioperative death unrelated to the FDD were excluded. Twenty-six (87 %) of the 30 dogs survived. Sixteen (53 %) dogs were able to retain the FDD for more than 3 weeks until 82 days. The autopsy findings revealed that four (15 %) dogs showed colonic wall erosions and mucosal scarring respectively at the band fixation area without evidence of serious septic complications. The surviving dogs retained the FDD for more than 6 days. Mortality occurred in four of the five dogs that expelled the FDD within three postoperative days. A closed abscess cavity as the evidence of anastomotic leakage was noted in seven (23 %) of the surviving dogs.
Conclusions: The newly designed fecal diverting device can be retained for more than 3 weeks until 82 days without any serious complications. The FDD may prevent sepsis in case of anastomotic leakage if it is retained for more than 6 days.
Figures
References
-
- Guenaga KF, Matos D, Castro AA, Atallah AN, Wille-Jorgensen P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst Rev. 2011;9:CD001544. - PubMed
-
- Montedori A, Cirocchi R, Farinella E, Sciannameo F, Abraha I. Covering ileo- or colostomy in anterior resection for rectal carcinoma. Cochrane Database Syst Rev. 2010;5:CD006878. - PubMed
-
- Ravo B, Ger R. A preliminary report on the intracolonic bypass as an alternative to a temporary colostomy. Surg Gynecol Obstet. 1984;159:541–545. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
