

Osteochondritis dissecans knee histology studies have variable findings and theories of etiology
- PMID: 23054514
- PMCID: PMC3586021
- DOI: 10.1007/s11999-012-2619-6
Osteochondritis dissecans knee histology studies have variable findings and theories of etiology
Abstract
Background: Although many etiological theories have been proposed for osteochondritis dissecans (OCD), its etiology remains unclear. Histological analysis of the articular cartilage and subchondral bone tissues of OCD lesions can provide useful information about the cellular changes and progression of OCD. Previous research is predominantly comprised of retrospective clinical studies from which limited conclusions can be drawn.
Questions/purposes: The purposes of this study were threefold: (1) Is osteonecrosis a consistent finding in OCD biopsy specimens? (2) Is normal articular cartilage a consistent finding in OCD biopsy specimens? (3) Do histological studies propose an etiology for OCD based on the tissue findings?
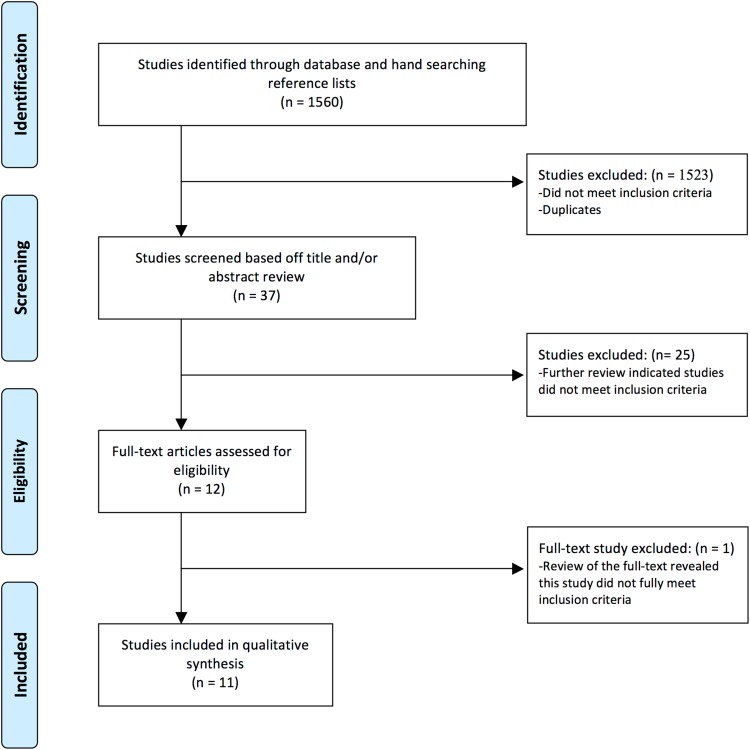
Methods: We searched the PubMed, Embase, and CINAHL databases for studies that conducted histological analyses of OCD lesions of the knee and identified 1560 articles. Of these, 11 met our inclusion criteria: a study of OCD lesions about the knee, published in the English language, and performed a histological analysis of subchondral bone and articular cartilage. These 11 studies were assessed for an etiology proposed in the study based on the study findings.
Results: Seven of 11 studies reported subchondral bone necrosis. Four studies reported normal articular cartilage, two studies reported degenerated or irregular articular cartilage, and five studies found a combination of normal and degenerated or irregular articular cartilage. Five studies proposed trauma or repetitive stress and two studies proposed poor blood supply as possible etiologies.
Conclusions: We found limited research on histological analysis of OCD lesions of the knee. Future studies with consistent methodology are necessary to draw major conclusions about the histology and progression of OCD lesions. Inconsistent histologic findings have resulted in a lack of consensus regarding the presence of osteonecrosis, whether the necrosis is primary or secondary, the association of cartilage degeneration, and the etiology of OCD. Such studies could use a standardized grading system to allow better comparison of findings.
Figures
References
-
- Cahill BR. Osteochondritis dissecans of the knee: treatment of juvenile and adult forms. J Am Acad Orthop Surg. 1995;3:237–247. - PubMed
-
- Campbell CJ, Ranawat CS. Osteochondritis dissecans: the question of etiology. J Trauma. 1966;6:201–221. - PubMed
-
- Enneking WF. Clinical Musculoskeletal Pathology. 1990. University Press of Florida. Available at: http://search.ebscohost.com/login.aspx?direct=true&db=nlebk&AN=20727&sit.... Accessed December 15, 2011.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
