

Estrogen receptor status in relation to risk of contralateral breast cancer-a population-based cohort study
- PMID: 23056335
- PMCID: PMC3466301
- DOI: 10.1371/journal.pone.0046535
Estrogen receptor status in relation to risk of contralateral breast cancer-a population-based cohort study
Abstract
Background: It is unclear whether estrogen receptor (ER)-status of first primary breast cancer is associated with risk of metachronous (non-simultaneous) contralateral breast cancer (CBC), and to what extent endocrine therapy affects this association.
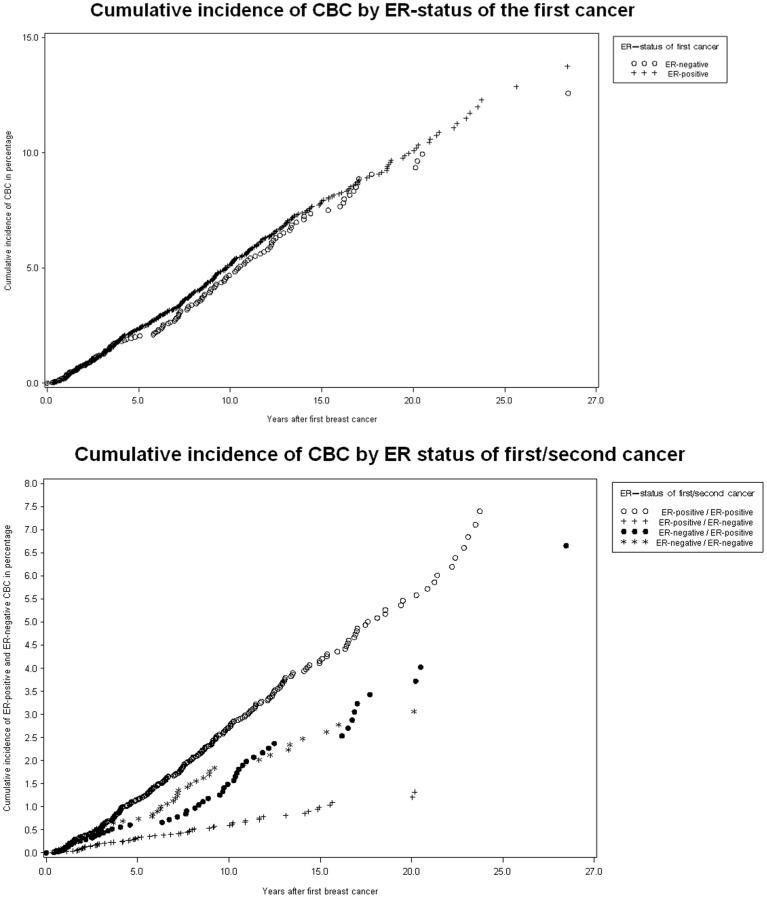
Methods: We studied the effect of ER-status of the first cancer on the risk of CBC overall, and for different ER-subtypes of CBC, using a large, population-based cohort. The cohort consisted of all women diagnosed with breast cancer in the Stockholm region 1976-2005; 25715 patients, of whom 940 suffered CBC. The relative risk was analyzed mainly using standardized incidence ratios (SIR).
Results: Women with breast cancer had a doubled risk of CBC compared to the risk of breast cancer in the general female population (SIR: 2.22 [2.08-2.36]), for women with a previous ER-positive cancer: SIR=2.30 (95% CI:2.11-2.50) and for women with a previous ER-negative cancer: SIR=2.17 (95% CI:1.82-2.55). The relative risk of ER-positive and ER-negative CBC was very similar for women with ER-positive first cancer (SIR=2.02 [95%CI: 1.80-2.27] and SIR=1.89 [95%CI: 1.46-2.41] respectively) while for patients with ER-negative first cancer the relative risk was significantly different (SIR=1.27 [95% CI:0.94-1.68] for ER-positive CBC and SIR=4.96 [95%CI:3.67-6.56] for ER-negative CBC). Patients with ER-positive first cancer who received hormone therapy still had a significantly higher risk of CBC than the risk of breast cancer for the general female population (SIR=1.74 [95% CI:1.47-2.03]).
Conclusion: The risk of CBC for a breast cancer patient is increased to about two-fold, compared to the risk of breast cancer in the general female population. This excess risk decreases, but does not disappear, with adjuvant endocrine therapy. Patients with ER-positive first cancers have an increased risk for CBC of both ER subtypes, while patients with ER-negative first cancer have a specifically increased risk of ER-negative CBC.
Conflict of interest statement
Figures
References
-
- Fowble B, Hanlon A, Freedman G, Nicolaou N, Anderson P (2001) Second cancers after conservative surgery and radiation for stages I–II breast cancer: identifying a subset of women at increased risk. Int J Radiat Oncol Biol Phys 51: 679–690. - PubMed
-
- Hankey BF, Curtis RE, Naughton MD, Boice JD Jr, Flannery JT (1983) A retrospective cohort analysis of second breast cancer risk for primary breast cancer patients with an assessment of the effect of radiation therapy. J Natl Cancer Inst 70: 797–804. - PubMed
-
- Healey EA, Cook EF, Orav EJ, Schnitt SJ, Connolly JL, et al. (1993) Contralateral breast cancer: clinical characteristics and impact on prognosis. J Clin Oncol 11: 1545–1552. - PubMed
-
- Hill-Kayser CE, Harris EE, Hwang WT, Solin LJ (2006) Twenty-year incidence and patterns of contralateral breast cancer after breast conservation treatment with radiation. Int J Radiat Oncol Biol Phys 66: 1313–1319. - PubMed
-
- Robbins GF (1964) Bilateral primary breast cancer: a prospective clinicopathological study. Cancer 17: 1501–1527. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
