

Adenovirus respiratory tract infections in Peru
- PMID: 23056519
- PMCID: PMC3466214
- DOI: 10.1371/journal.pone.0046898
Adenovirus respiratory tract infections in Peru
Abstract
Background: Currently, there is a paucity of data regarding human adenovirus (HAdv) circulation in Andean regions of South America. To address this shortcoming, we report the clinical, phylogenetic, and epidemiologic characteristics of HAdv respiratory tract infection from a large sentinel surveillance study conducted among adults and children in Peru.
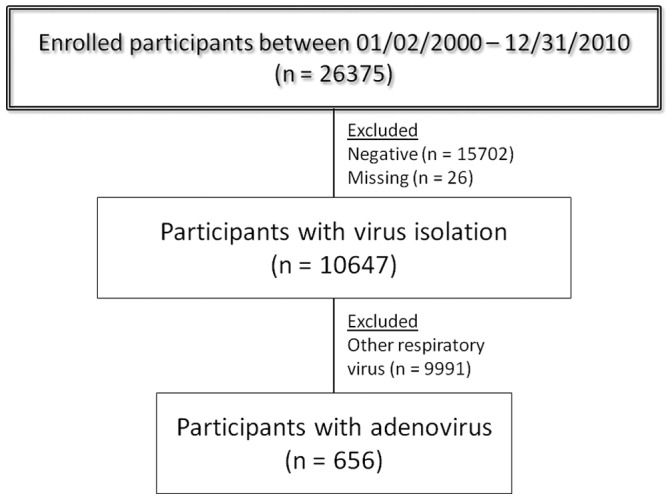
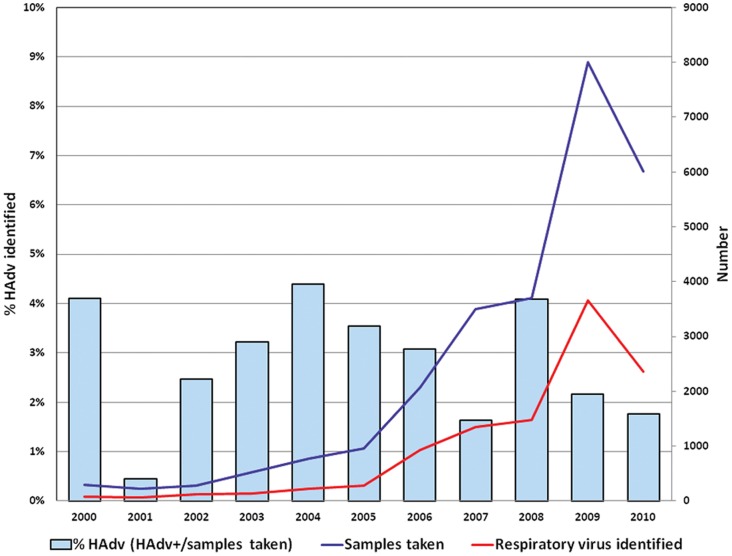
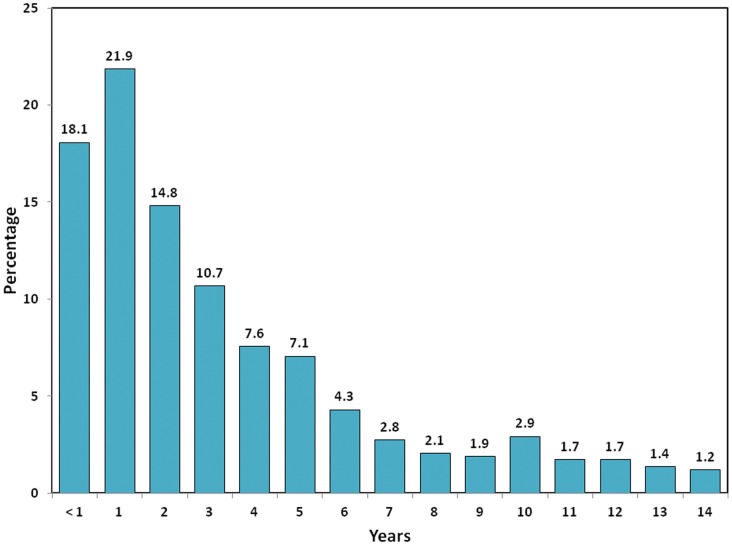
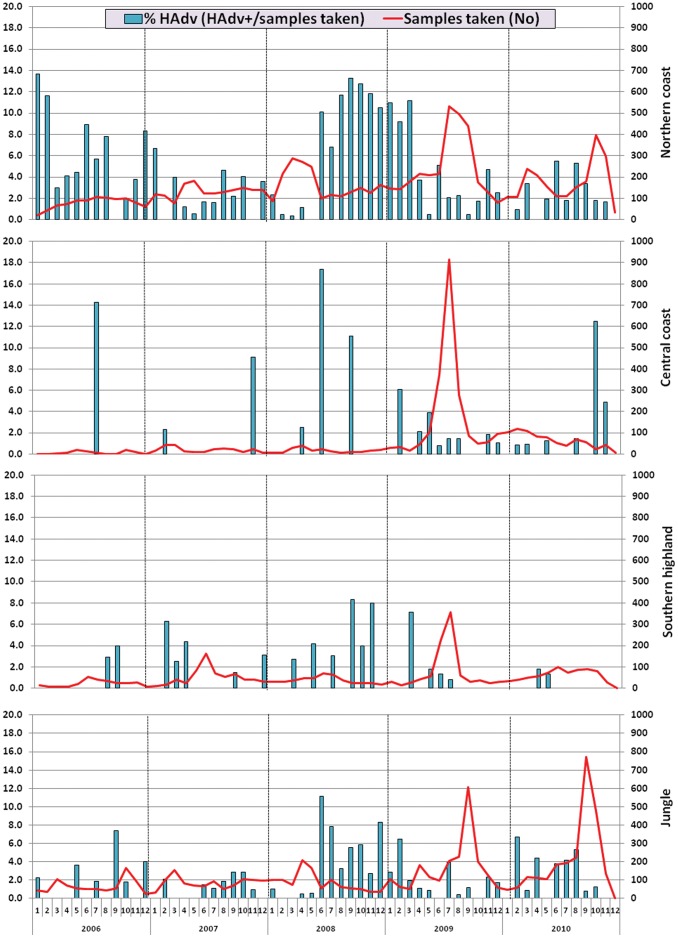
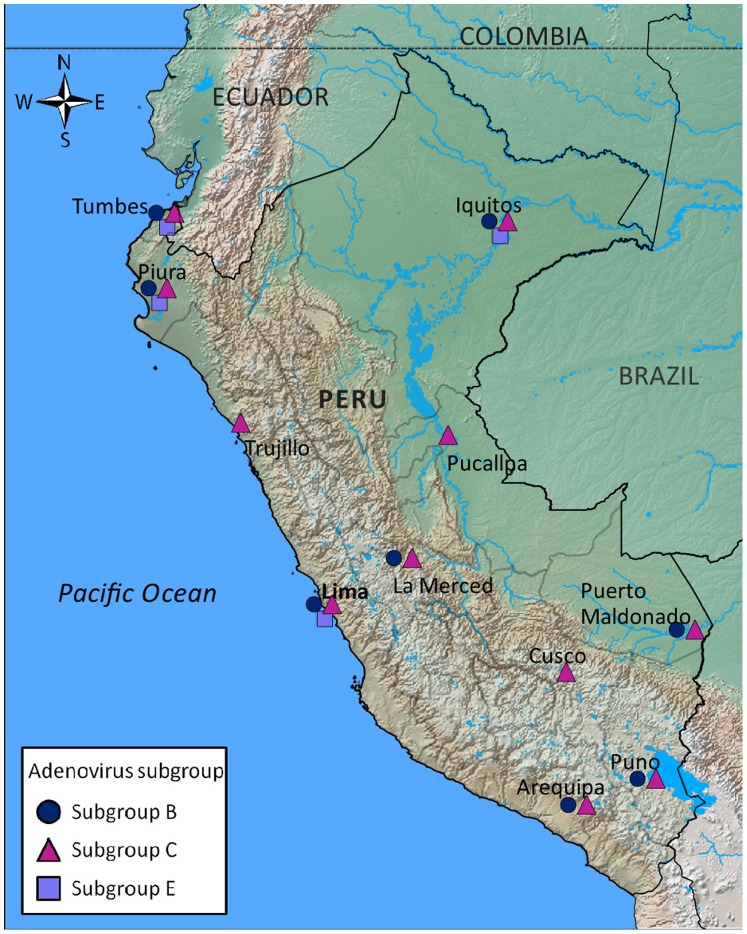
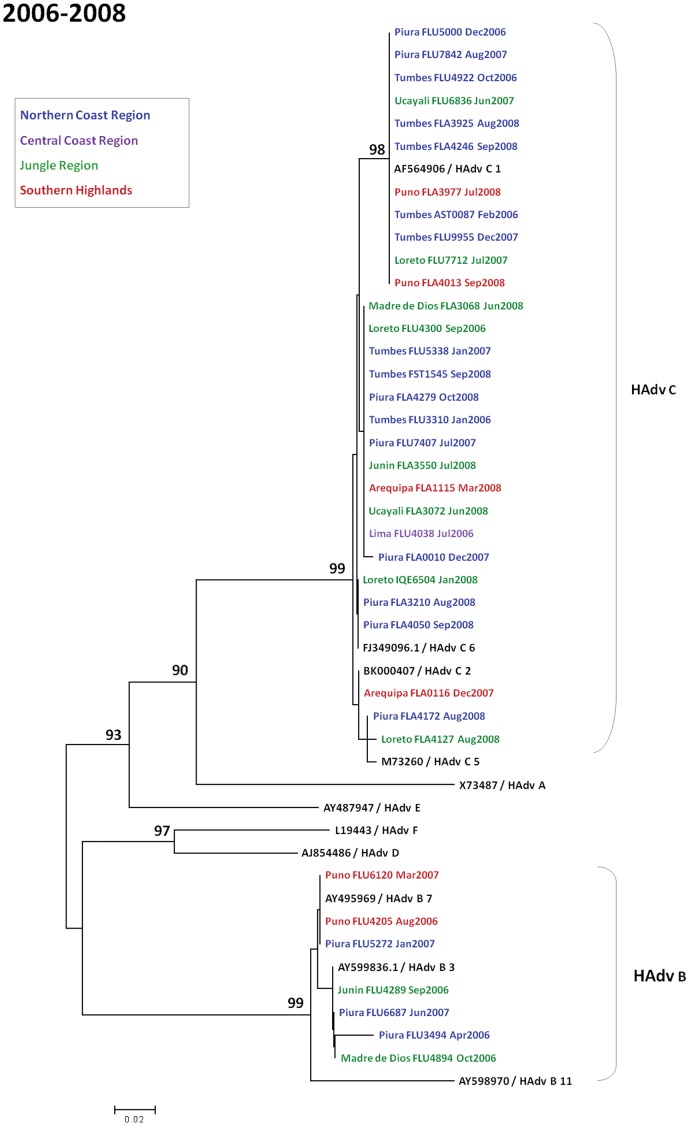
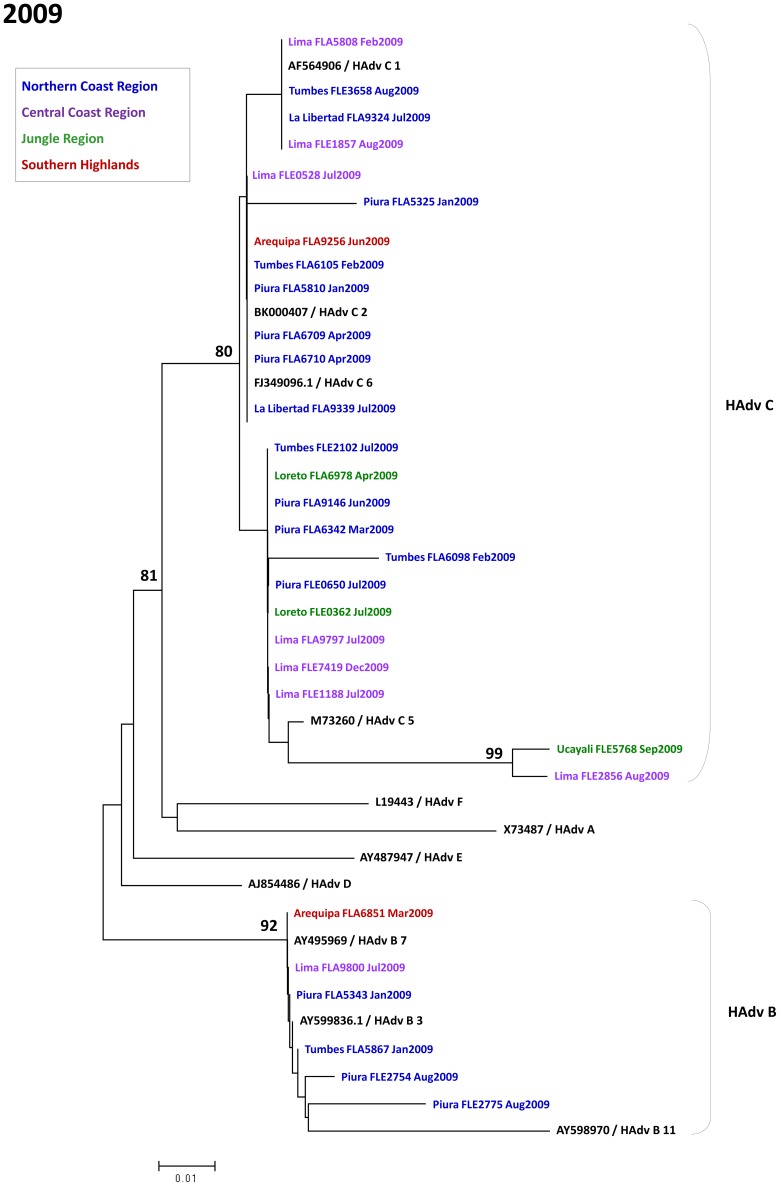
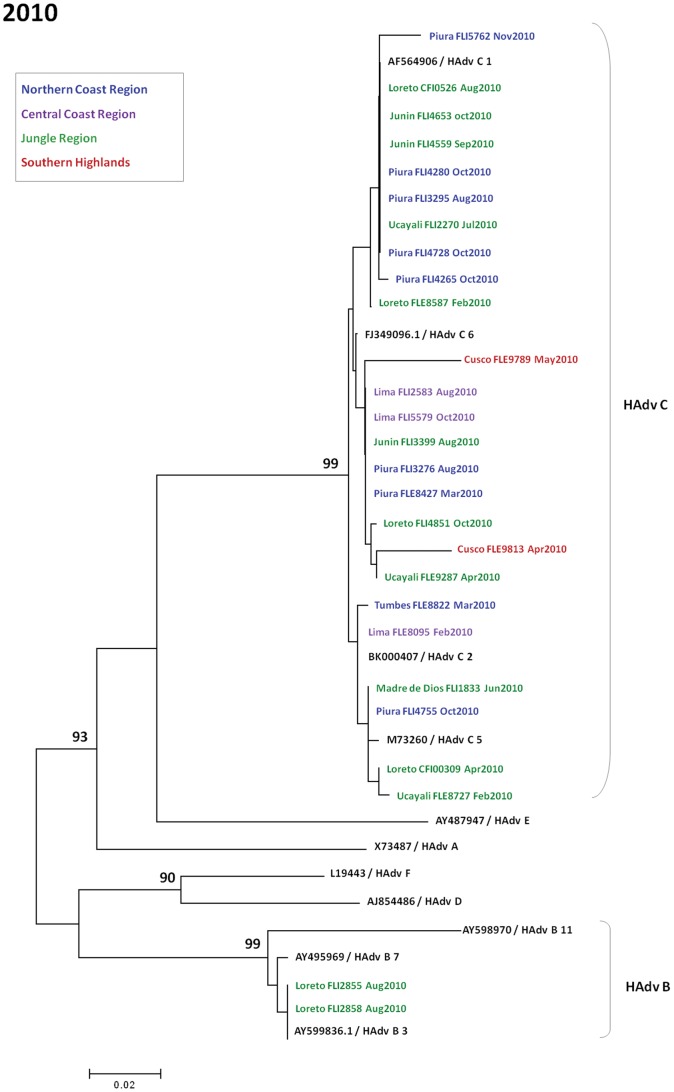
Methods/principal findings: Oropharyngeal swabs were collected from participants visiting any of 38 participating health centers, and viral pathogens were identified by immunofluorescence assay in cell culture. In addition, molecular characterization was performed on 226 randomly selected HAdv samples. Between 2000 and 2010, a total of 26,375 participants with influenza-like illness (ILI) or severe acute respiratory infection (SARI) were enrolled in the study. HAdv infection was identified in 2.5% of cases and represented 6.2% of all viral pathogens. Co-infection with a heterologous virus was found in 15.5% of HAdv cases. HAdv infection was largely confined to children under the age of 15, representing 88.6% of HAdv cases identified. No clinical characteristics were found to significantly distinguish HAdv infection from other respiratory viruses. Geographically, HAdv infections were more common in sites from the arid coastal regions than in the jungle or highland regions. Co-circulation of subgroups B and C was observed each year between 2006 and 2010, but no clear seasonal patterns of transmission were detected.
Conclusions/significance: HAdv accounted for a significant fraction of those presenting with ILI and SARI in Peru and tended to affect the younger population disproportionately. Longitudinal studies will help better characterize the clinical course of patients with HAdv in Peru, as well as determine the role of co-infections in the evolution of illness.
Conflict of interest statement
Figures
References
-
- Bunchen-Osmond C (2007) Taxonomy and Classification of Viruses. In: Murray P, editor. Manual of Clinical Microbiology. 9th ed. Washington D.C: ASM Press. pp. 1273–1283.
-
- Flint S, Enquist L, Racaniello V, Skalka A (2009) Adenoviruses. In: Flint S, Enquist L, Racaniello V, Skalka A, editors. Principles of virology. Third ed. Washington D.C: ASM Press. pp. 502.
-
- Han BK, Son JA, Yoon HK, Lee SI (1998) Epidemic adenoviral lower respiratory tract infection in pediatric patients: radiographic and clinical characteristics. AJR Am J Roentgenol 170: 1077–1080. - PubMed
-
- Choi EH, Lee HJ, Kim SJ, Eun BW, Kim NH, et al. (2006) Ten-year analysis of adenovirus type 7 molecular epidemiology in Korea, 1995–2004: implication of fiber diversity. J Clin Virol 35: 388–393. - PubMed
-
- Mufson MA, Belshe RB (1976) A review of adenoviruses in the etiology of acute hemorrhagic cystitis. J Urol 115: 191–194. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
