

Aberrant drug-related behaviors: unsystematic documentation does not identify prescription drug use disorder
- PMID: 23057631
- PMCID: PMC3501607
- DOI: 10.1111/j.1526-4637.2012.01497.x
Aberrant drug-related behaviors: unsystematic documentation does not identify prescription drug use disorder
Abstract
Objective: No evidence-based methods exist to identify prescription drug use disorder (PDUD) in primary care (PC) patients prescribed controlled substances. Aberrant drug-related behaviors (ADRBs) are suggested as a proxy. Our objective was to determine whether ADRBs documented in electronic medical records (EMRs) of patients prescribed opioids and benzodiazepines could serve as a proxy for identifying PDUD.
Design: A cross-sectional study of PC patients at an urban, academic medical center.
Subjects: Two hundred sixty-four English-speaking patients (ages 18-60) with chronic pain (≥3 months), receiving ≥1 opioid analgesic or benzodiazepine prescription in the past year, were recruited during outpatient PC visits.
Outcome measures: Composite International Diagnostic Interview defined Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) diagnoses of past year PDUD and no disorder. EMRs were reviewed for 15 prespecified ADRBs (e.g., early refill, stolen medications) in the year before and after study entry. Fisher's exact test compared frequencies of each ADRB between participants with and without PDUD.
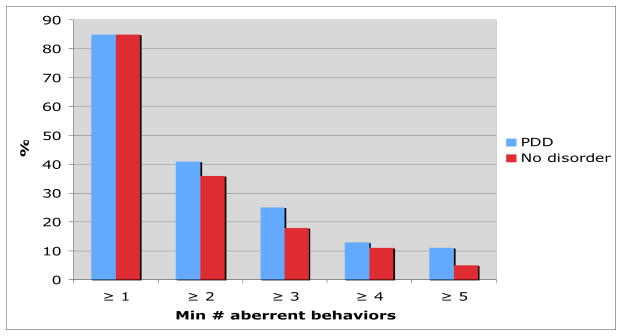
Results: Sixty-one participants (23%) met DSM-IV PDUD criteria and 203 (77%) had no disorder; 85% had one or more ADRB documented. Few differences in frequencies of individual behaviors were noted between groups, with only "appearing intoxicated or high" documented more frequently among participants with PDUD (N = 10, 16%) vs no disorder (N = 8, 4%), P = 0.002. The only common ADRB, "emergency visit for pain," did not discriminate between those with and without the disorder (82% PDUD vs 78% no disorder, P = 0.6).
Conclusions: EMR documentation of ADRBs is common among PC patients prescribed opioids or benzodiazepines, but unsystematic clinician documentation does not identify PDUDs. Evidence-based approaches are needed.
Wiley Periodicals, Inc.
Conflict of interest statement
The authors all report no conflicts of interest. R. Saitz is a consultant for Medical Directions Inc. and BMJ Publishing Group
Figures
References
-
- Gureje O, Von Korff M, Simon GE, Gater R. Persistent pain and well-being: A world health organization study in primary care.[erratum appears in JAMA 1998 oct 7;280(13):1142] JAMA. 1998;280(2):147–51. - PubMed
-
- Marks RM, Sachar EJ. Undertreatment of medical inpatients with narcotic analgesics. Annals of Internal Medicine. 1978;78:173–81. - PubMed
-
- Cicero TJ, Inciardi JA, Munoz A. Trends in abuse of oxycontin and other opioid analgesics in the united states: 2002–2004. J Pain. 2005;6(10):662–72. - PubMed
-
- Bell J. The global diversion of pharmaceutical drugs: Opiate treatment and the diversion of pharmaceutical opiates: A clinician’s perspective. Addiction. 2010;105(9):1531–7. - PubMed
-
- Centers for Disease Control and Prevention (CDC) Emergency department visits involving nonmedical use of selected prescription drugs - united states, 2004–2008. MMWR Morb Mortal Wkly Rep. 2010;59(23):705–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
