

Coronary vascular dysfunction and prognosis in patients with chronic kidney disease
- PMID: 23058070
- PMCID: PMC3471090
- DOI: 10.1016/j.jcmg.2012.06.007
Coronary vascular dysfunction and prognosis in patients with chronic kidney disease
Abstract
Objectives: This study sought to evaluate whether impaired vasodilator function, an early manifestation of coronary artery disease, which precedes angiographic stenosis, accounts for increased risk among patients with moderate to severe renal dysfunction.
Background: Patients with renal dysfunction are at increased risk of adverse cardiac outcomes, even in the absence of overt myocardial ischemia or infarction.
Methods: We included 866 consecutive patients with moderate to severe renal dysfunction referred for rest and stress myocardial perfusion positron emission tomography and followed them for a median of 1.28 years (interquartile range: 0.64 to 2.34). Regional myocardial perfusion abnormalities were assessed by semiquantitative visual analysis of positron emission tomography images. Rest and stress myocardial blood flow were calculated using factor analysis and a 2-compartment kinetic model; they were also used to compute coronary flow reserve (stress/rest myocardial blood flow). The primary endpoint was cardiac death.
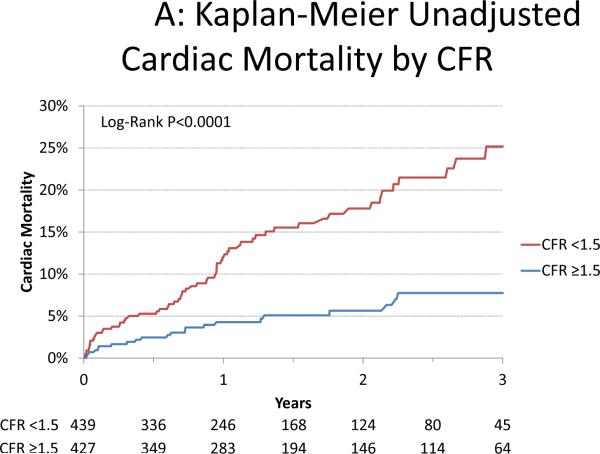
Results: Overall, 3-year cardiac mortality was 16.2%. After adjusting for clinical risk, left ventricular ejection fraction, as well as the magnitude of scar and/or ischemia, coronary flow reserve below the median (<1.5) was associated with a 2.1-fold increase in the risk of cardiac death (95% confidence interval [CI]: 1.3 to 3.5, p = 0.004). Incorporation of coronary flow reserve into cardiac death risk assessment models resulted in an increase in the C-index from 0.75 to 0.77 (p = 0.05) and in a net reclassification improvement of 0.142 (95% CI: 0.076 to 0.219). Among patients at intermediate risk based on all data other than coronary flow reserve, the net reclassification improvement was 0.489 (95% CI: 0.192 to 0.836). Corresponding improvements in risk assessment for mortality from any cause were also demonstrated.
Conclusions: The presence of coronary vascular dysfunction in patients with moderate to severe renal dysfunction, as assessed by positron emission tomography, is a powerful, independent predictor of cardiac mortality and provides meaningful incremental risk stratification over conventional markers of clinical risk.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures





Comment in
-
Enhancing risk prediction with PET coronary flow reserve: can it be clinically useful?JACC Cardiovasc Imaging. 2012 Oct;5(10):1035-6. doi: 10.1016/j.jcmg.2012.08.005. JACC Cardiovasc Imaging. 2012. PMID: 23058071 No abstract available.
References
-
- U.S. Renal Data System . USRDS 2010 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda, MD: 2010. Available at: http://www.usrds.org/adr.htm.
-
- Shin D-H, Choi D-J, Youn T-J, et al. Comparison of Contrast-Induced Nephrotoxicity of Iodixanol and Iopromide in Patients With Renal Insufficiency Undergoing Coronary Angiography. The American Journal of Cardiology. 2011;108(2):189–194. - PubMed
-
- Rihal CS, Textor SC, Grill DE, et al. Incidence and Prognostic Importance of Acute Renal Failure After Percutaneous Coronary Intervention. Circulation. 2002;105(19):2259–2264. - PubMed
-
- Gruberg L, Mintz GS, Mehran R, et al. The prognostic implications of further renal function deterioration within 48 h of interventional coronary procedures in patients with pre-existent chronic renal insufficiency. Journal of the American College of Cardiology. 2000;36(5):1542–1548. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
