

Mortality rates in smokers and nonsmokers in the presence or absence of coronary artery calcification
- PMID: 23058072
- PMCID: PMC4405129
- DOI: 10.1016/j.jcmg.2012.02.017
Mortality rates in smokers and nonsmokers in the presence or absence of coronary artery calcification
Erratum in
- JACC Cardiovasc Imaging. 2013 Jun;6(6):747
Abstract
Objectives: The aim of this study was to further explore the interplay between smoking status, coronary artery calcium (CAC), and all-cause mortality.
Background: Prior studies have not directly compared the relative prognostic impact of CAC in smokers versus nonsmokers. In particular, although a calcium score of zero (CAC = 0) is a known favorable prognostic marker, whether smokers with CAC = 0 have as good a prognosis as nonsmokers with CAC = 0 is unknown. Given that computed tomography (CT) screening for lung cancer appears effective in smokers, the relative prognostic implications of visualizing any CAC versus no CAC on such screening also deserve study.
Methods: Our study cohort consisted of 44,042 asymptomatic individuals referred for noncontrast cardiac CT (age 54 ± 11 years, 54% men). Subjects were followed for a mean of 5.6 years. The primary endpoint was all-cause mortality.
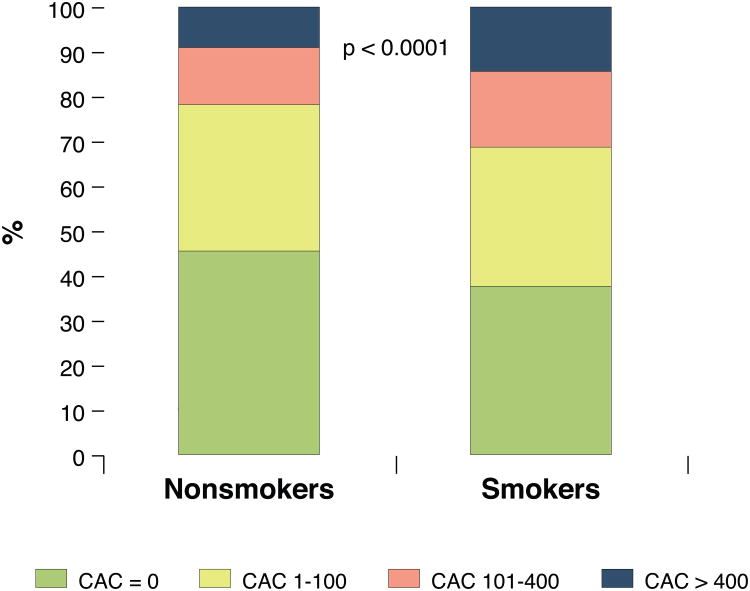
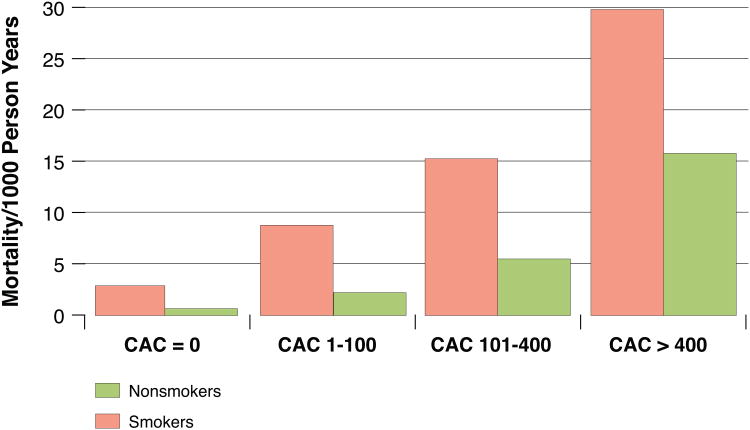
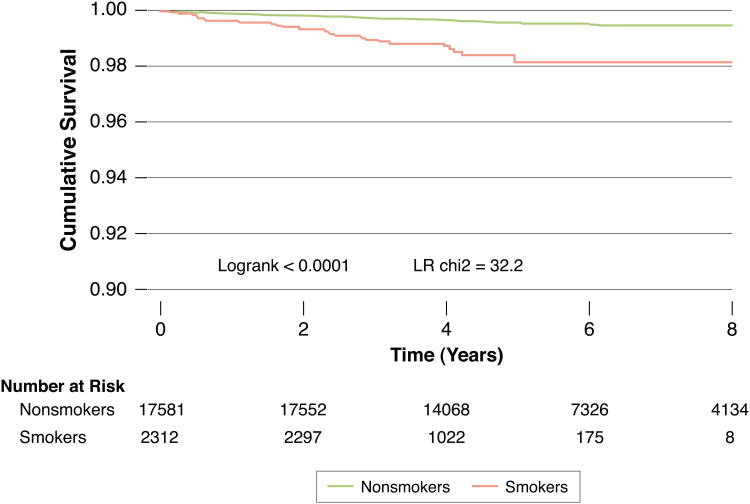
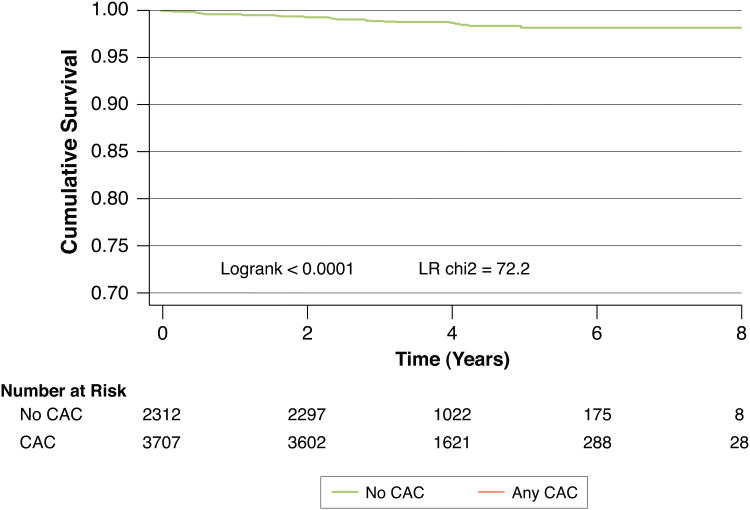
Results: Approximately 14% (n = 6,020) of subjects were active smokers at enrollment. There were 901 deaths (2.05%) overall, with increased mortality in smokers versus nonsmokers (4.3% vs. 1.7%, p < 0.0001). Smoking remained a risk factor for mortality across increasing strata of CAC scores (1 to 100, 101 to 400, and >400). At each stratum of elevated CAC score, mortality in smokers was consistently higher than mortality in nonsmokers from the CAC stratum above. In multivariable analysis within these strata, we found mortality hazard ratios of 3.8 (95% confidence interval [CI]: 2.8 to 5.2), 3.5 (95% CI: 2.6 to 4.9), and 2.7 (95% CI: 2.1 to 3.5), respectively, in smokers compared with nonsmokers. However, among the 19,898 individuals with CAC = 0, the mortality hazard ratio for smokers without CAC was 3.6 (95% CI: 2.3 to 5.7), compared with nonsmokers without CAC.
Conclusions: Smoking is a risk factor for death across the entire spectrum of subclinical coronary atherosclerosis. Smokers with any CAC had significantly higher mortality than smokers without CAC, a finding with implications for smokers undergoing lung cancer CT-based screening. However, the absence of CAC might not be as useful a "negative risk factor" in active smokers, because this group has mortality rates similar to nonsmokers with mild-to-moderate atherosclerosis.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Lloyd-Jones D, Adams RJ, Brown TM, et al. Heart disease and stroke statistics--2010 update: a report from the American Heart Association. Circulation. 2010 Feb 23;121(7):e46–e215. - PubMed
-
- McElvaney NG. Smoking ban--made in Ireland, for home use and for export. N Engl J Med. 2004 May 27;350(22):2231–2233. - PubMed
-
- Celermajer DS, Sorensen KE, Georgakopoulos D, et al. Cigarette smoking is associated with dose-related and potentially reversible impairment of endothelium-dependent dilation in healthy young adults. Circulation. 1993 Nov;88(5 Pt 1):2149–2155. - PubMed
-
- Ambrose JA, Barua RS. The pathophysiology of cigarette smoking and cardiovascular disease: an update. J Am Coll Cardiol. 2004 May 19;43(10):1731–1737. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
