

Bortezomib in the rapid reduction of high sustained antibody titers in disorders treated with therapeutic protein: lessons learned from Pompe disease
- PMID: 23060045
- PMCID: PMC3744338
- DOI: 10.1038/gim.2012.110
Bortezomib in the rapid reduction of high sustained antibody titers in disorders treated with therapeutic protein: lessons learned from Pompe disease
Abstract
Purpose: High sustained antibody titers complicate many disorders treated with a therapeutic protein, including those treated with enzyme replacement therapy, such as Pompe disease. Although enzyme replacement therapy with alglucosidase alfa (Myozyme) in Pompe disease has improved the prognosis of this otherwise lethal disorder, patients who develop high sustained antibody titers to alglucosidase alfa enter a prolonged phase of clinical decline resulting in death despite continued enzyme replacement therapy. Clinically effective immune-tolerance induction strategies have yet to be described in the setting of an entrenched immune response characterized by high sustained antibody titers, wherein antibody-producing plasma cells play an especially prominent role.
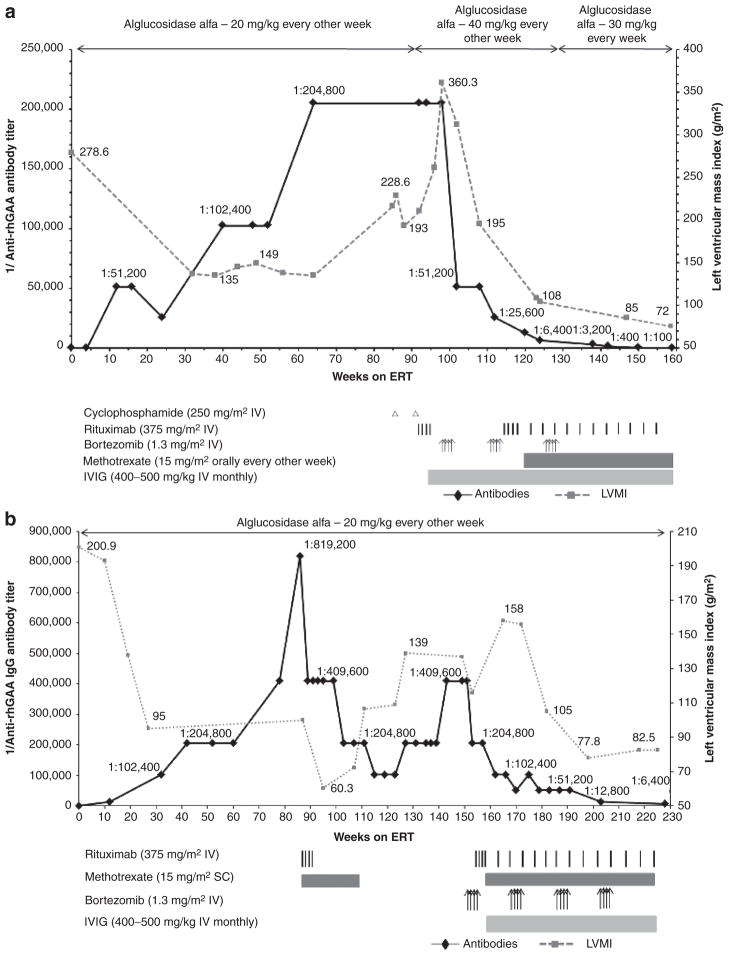
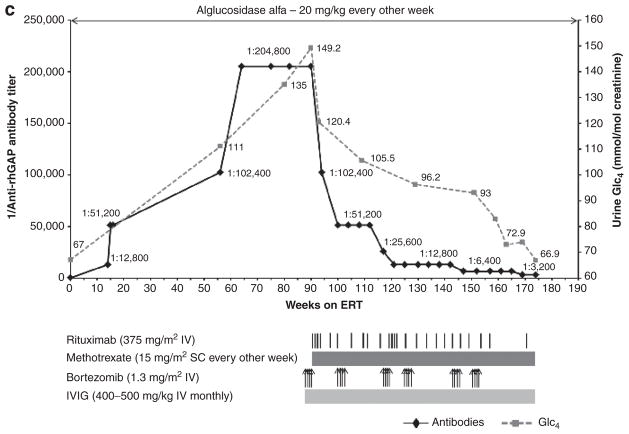
Methods: We treated three patients with infantile Pompe disease experiencing marked clinical decline due to high sustained antibody titers. To target the plasma cell source of high sustained antibody titers, a regimen based on bortezomib (Velcade) was used in combination with rituximab, methotrexate, and intravenous immunoglobulin.
Results: The treatment regimen was well tolerated, with no obvious side effects. Patient 1 had a 2,048-fold, and patients 2 and 3 each had a 64-fold, reduction in anti-alglucosidase alfa antibody titer, with concomitant sustained clinical improvement.
Conclusion: The addition of bortezomib to immunomodulatory regimens is an effective and safe treatment strategy in infantile Pompe disease, with potentially broader clinical implications.
Conflict of interest statement
The other authors declare no conflict of interest.
Figures
References
-
- Porter S. Human immune response to recombinant human proteins. J Pharm Sci. 2001;90:1–11. - PubMed
-
- Amalfitano A, Bengur AR, Morse RP, et al. Recombinant human acid alphaglucosidase enzyme therapy for infantile glycogen storage disease type II: results of a phase I/II clinical trial. Genet Med. 2001;3:132–138. - PubMed
-
- Hollak CE, Linthorst GE. Immune response to enzyme replacement therapy in Fabry disease: impact on clinical outcome? Mol Genet Metab. 2009;96:1–3. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
