

Nimotuzumab prolongs survival in patients with malignant gliomas: A phase I/II clinical study of concomitant radiochemotherapy with or without nimotuzumab
- PMID: 23060940
- PMCID: PMC3460247
- DOI: 10.3892/etm.2012.555
Nimotuzumab prolongs survival in patients with malignant gliomas: A phase I/II clinical study of concomitant radiochemotherapy with or without nimotuzumab
Abstract
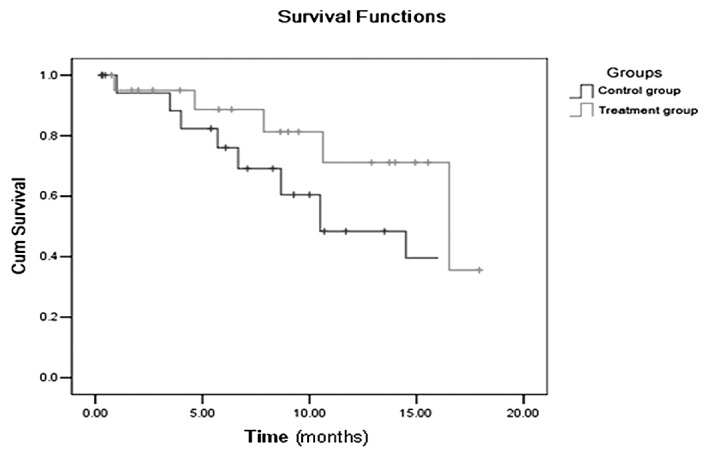
The present study aimed to determine whether nimotuzumab enhances the effect of radiochemotherapy in malignant gliomas. Patients (n=41) with malignant gliomas were divided into 20 cases (treatment group) in which nimotuzumab plus radiochemotherapy were offered and 21 cases (control group) in which placebo and radiochemotherapy were administered to the patients. The response to treatment was evaluated according to the Response Evaluation Criteria in Solid Tumors, the Kaplan-Meier method was used to calculate the mean and median survival times and 1-year survival rate, and the log-rank test and the Chi-square test were used to analyze the difference in the survival and response rate between the treatment and control groups. The mean survival times of the treatment and control groups were 14.3 and 10.4 months and the median survival times of the treatment and control groups were 16.5 and 10.5 months, respectively. The 1-year survival rates of the treatment and control groups were 81.3 and 69.1%, respectively, with no significant difference (P>0.05). The objective response rates of the treatment and control groups were 70.0 and 52.4%, respectively, with no significant difference (P>0.05). In conclusion, there was a trend towards improved treatment efficacy of radiochemotherapy combined with nimotuzumab against malignant gliomas. This study demonstrated that the use of nimotuzumab combined with radiotherapy and concomitant temozolomide chemotherapy is effective for malignant gliomas.
Figures
References
-
- Counsell CE, Grant R. Incidence studies of primary and secondary intracranial tumors: a systematic review of their methodology and results. J Neurooncol. 1998;37:241–250. - PubMed
-
- Nazzaro JM, Neuwelt EA. The role of surgery in the management of supratentorial intermediate and high-grade astrocytomas in adults. J Neurosurg. 1990;73:331–344. - PubMed
-
- Wood JR, Green SB, Shapiro WR. The prognostic importance of tumor size in malignant gliomas: a computed tomographic scan study by the Brain Tumor Cooperative Group. J Clin Oncol. 1988;6:338–343. - PubMed
-
- Albert FK, Forsting M, Sartor K, Adams HP, Kunze S. Early postoperative magnetic resonance imaging after resection of malignant glioma: objective evaluation of residual tumor and its influence on regrowth and prognosis. Neurosurgery. 1994;34:45–61. - PubMed
-
- Devaux BC, O’Fallon JR, Kelly PJ. Resection, biopsy, and survival in malignant glial neoplasms. A retrospective study of clinical parameters, therapy, and outcome. J Neurosurg. 1993;78:767–775. - PubMed
LinkOut - more resources
Full Text Sources