

Ventriculoperitoneal shunting versus endoscopic third ventriculostomy in the treatment of patients with hydrocephalus related to metastasis
- PMID: 23061013
- PMCID: PMC3463839
- DOI: 10.4103/2152-7806.100185
Ventriculoperitoneal shunting versus endoscopic third ventriculostomy in the treatment of patients with hydrocephalus related to metastasis
Abstract
Background: Between 2005 and 2010, we treated patients with hydrocephalus related to cerebral metastases, who were not good candidates for surgical resection by either endoscopic third ventriculostomy (ETV) or ventriculoperitoneal shunting (VPS). Patients were excluded from ETV if they had a clinical history suggestive of non-obstructive hydrocephalus, including: (1) history of infection or ventricular hemorrhage and (2) leptomeningeal carcinomatosis. The rest of the patients were treated with VPS.
Methods: We analyzed the clinical outcome of these patient cohorts, to determine whether the efficacy of VPS was compromised due to a history of infection, ventricular hemorrhage, or leptomeningeal carcinomatosis, and compared these results to those patients who underwent ETV.
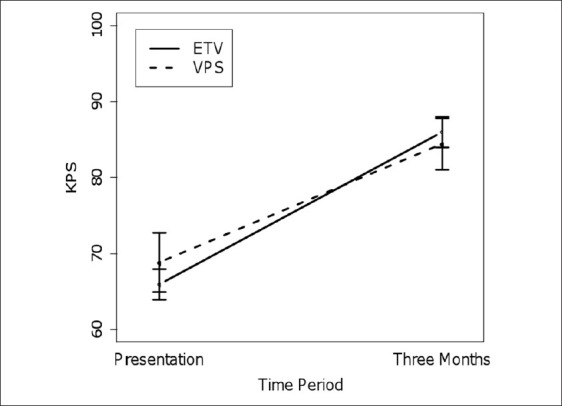
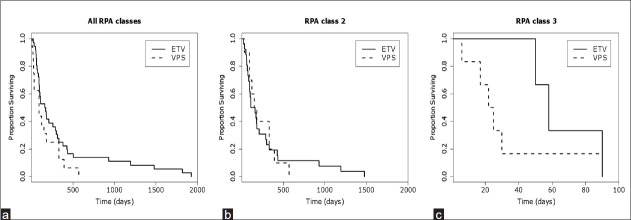
Results: Sixteen patients were treated with ETV and 36 patients were treated with VPS. The overall efficacy of symptomatic palliation was comparable in the ETV and VPS patients (ETV = 69%, VPS = 75%). In both groups, patients with more severe hydrocephalic symptoms such as nausea, vomiting, and lethargy were more likely to benefit from the procedure. The overall complication rate for the two groups was comparable (ETV = 12.6%, VPS = 19.4%), although the spectrum of complications differed. The overall survival, initial Karnofsky performance status (KPS), and three-month KPS, were similarly comparable (median survival: ETV 3 months, VPS 5.5 months; initial KPS: ETV = 66 ± 7, VPS = 69 ± 12; 3 months KPS: ETV = 86 ± 7, KPS = 84 ± 12).
Conclusion: VPS remains a reasonable option for poor RPA grade metastasis patients with hydrocephalus, even in the setting of a previous infection, hemorrhage, or in those with leptomeningeal disease. Optimal treatment of this population will involve the judicious consideration of the relative merits of VPS and ETV.
Keywords: Cerebral metastasis; Ventriculoperitoneal shunting; endoscopic third ventriculostomy; palliation.
Figures
Similar articles
-
Comparison of hydrocephalus metrics between infants successfully treated with endoscopic third ventriculostomy with choroid plexus cauterization and those treated with a ventriculoperitoneal shunt: a multicenter matched-cohort analysis.J Neurosurg Pediatr. 2018 Apr;21(4):339-345. doi: 10.3171/2017.10.PEDS17421. Epub 2018 Feb 2. J Neurosurg Pediatr. 2018. PMID: 29393809
-
Ventriculoperitoneal Shunt and Endoscopic Third Ventriculostomy for Hydrocephalus in Adult Patients With Brain Metastases.Cureus. 2025 Jan 20;17(1):e77707. doi: 10.7759/cureus.77707. eCollection 2025 Jan. Cureus. 2025. PMID: 39974223 Free PMC article.
-
Endoscopic third ventriculostomy for pediatric tumor-associated hydrocephalus.Neurosurg Focus. 2020 Jan 1;48(1):E5. doi: 10.3171/2019.10.FOCUS19725. Neurosurg Focus. 2020. PMID: 31896082
-
Re-endoscopic third ventriculostomy versus ventriculoperitoneal shunting in failed endoscopic third ventriculostomy in pediatric patients with hydrocephalus: A systematic review.Surg Neurol Int. 2025 May 30;16:205. doi: 10.25259/SNI_1111_2024. eCollection 2025. Surg Neurol Int. 2025. PMID: 40469369 Free PMC article. Review.
-
Endoscopic Third Ventriculostomy versus Ventriculoperitoneal Shunt in Patients with Obstructive Hydrocephalus: Meta-Analysis of Randomized Controlled Trials.World Neurosurg. 2019 Sep;129:334-340. doi: 10.1016/j.wneu.2019.04.255. Epub 2019 May 25. World Neurosurg. 2019. PMID: 31136836 Review.
Cited by
-
The role of radiosurgery in the acute management of fourth ventricle compression due to brain metastases.Surg Neurol Int. 2018 May 29;9:112. doi: 10.4103/sni.sni_387_17. eCollection 2018. Surg Neurol Int. 2018. PMID: 29930878 Free PMC article.
-
Cerebrospinal fluid diversion for leptomeningeal metastasis: palliative, procedural and oncologic outcomes.J Neurooncol. 2021 Sep;154(3):301-313. doi: 10.1007/s11060-021-03827-2. Epub 2021 Aug 18. J Neurooncol. 2021. PMID: 34406564 Free PMC article.
-
Characteristics and management of hydrocephalus in adult patients with cerebellar glioblastoma: lessons from a French nationwide series of 118 cases.Neurosurg Rev. 2022 Feb;45(1):683-699. doi: 10.1007/s10143-021-01578-2. Epub 2021 Jul 1. Neurosurg Rev. 2022. PMID: 34195892
-
Chinese Expert Consensus on Leptomeningeal Metastases of Lung Cancer.Thorac Cancer. 2025 Jun;16(11):e70088. doi: 10.1111/1759-7714.70088. Thorac Cancer. 2025. PMID: 40484812 Free PMC article.
-
Management of hydrocephalus in patients with leptomeningeal metastases: an ethical approach to decision-making.J Neurooncol. 2018 Oct;140(1):5-13. doi: 10.1007/s11060-018-2949-7. Epub 2018 Jul 18. J Neurooncol. 2018. PMID: 30022283 Free PMC article. Review.
References
-
- Brouwer AJ, Groenendaal F, van den Hoogen A, Verboon-Maciolek M, Hanlo P, Rademaker KJ, et al. Incidence of infections of ventricular reservoirs in the treatment of post-haemorrhagic ventricular dilatation: A retrospective study (1992-2003) Arch Dis Child Fetal Neonatal Ed. 2007;92:F41–3. - PMC - PubMed
-
- Bruinsma N, Stobberingh EE, Herpers MJ, Vles JS, Weber BJ, Gavilanes DA. Subcutaneous ventricular catheter reservoir and ventriculoperitoneal drain-related infections in preterm infants and young children. Clin Microbiol Infect. 2000;6:202–6. - PubMed
-
- Drake JM, Kulkarni AV, Kestle J. Endoscopic third ventriculostomy versus ventriculoperitoneal shunt in pediatric patients: A decision analysis. Childs Nerv Syst. 2009;25:467–72. - PubMed
-
- Farahmand D, Hilmarsson H, Hogfeldt M, Tisell M. Perioperative risk factors for short term shunt revisions in adult hydrocephalus patients. J Neurol Neurosurg Psychiatry. 2009;80:1248–53. - PubMed
LinkOut - more resources
Full Text Sources
