

"Time is brain" the Gifford factor - or: Why do some civilian gunshot wounds to the head do unexpectedly well? A case series with outcomes analysis and a management guide
- PMID: 23061014
- PMCID: PMC3463834
- DOI: 10.4103/2152-7806.100187
"Time is brain" the Gifford factor - or: Why do some civilian gunshot wounds to the head do unexpectedly well? A case series with outcomes analysis and a management guide
Abstract
Background: Review of intracranial gunshot wounds (GSWs) undergoing emergent neurosurgical intervention despite a very low Glasgow Coma Scale (GCS) score on admission in order to identify predictors of good outcome, with correlates to recent literature.
Methods: A retrospective review of select cases of GSWs presenting to our trauma center over the past 5 years with poor GCS requiring emergent neurosurgical intervention and a minimum of 1-year follow-up.
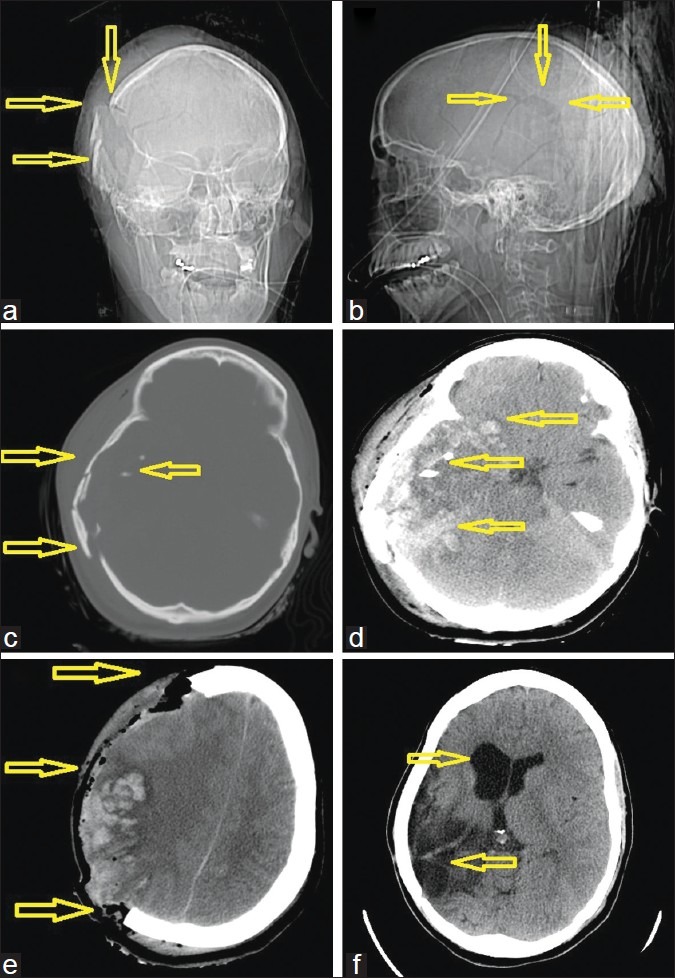
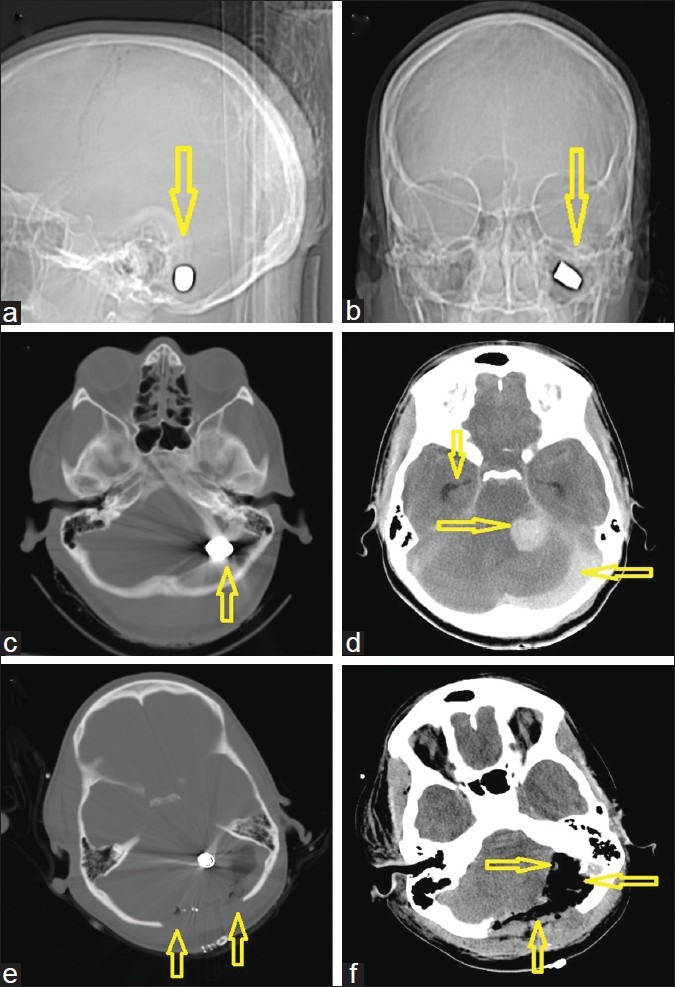
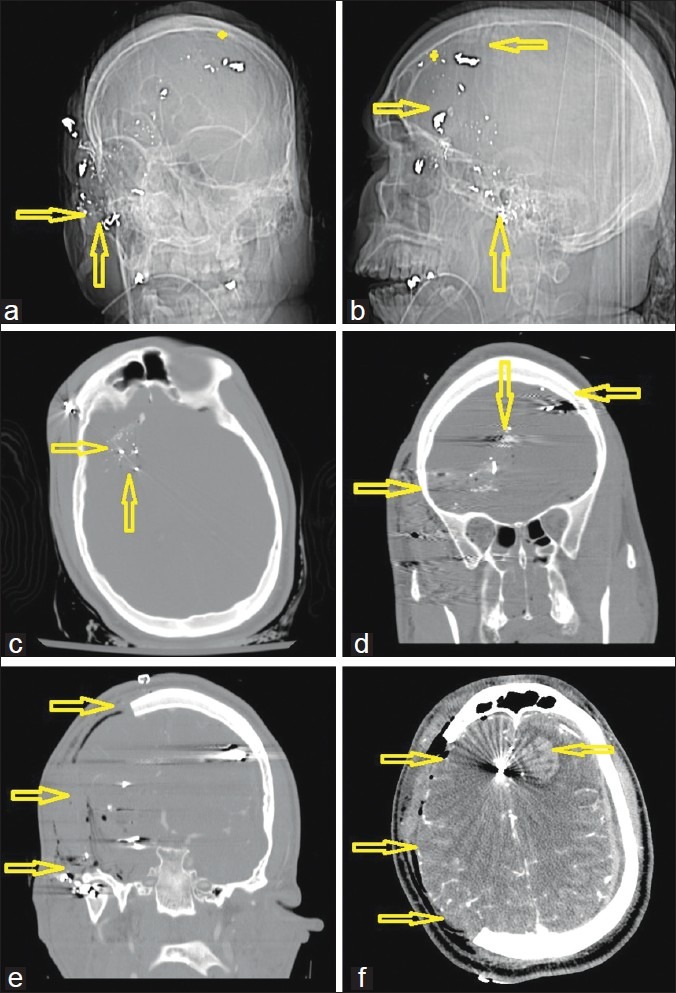
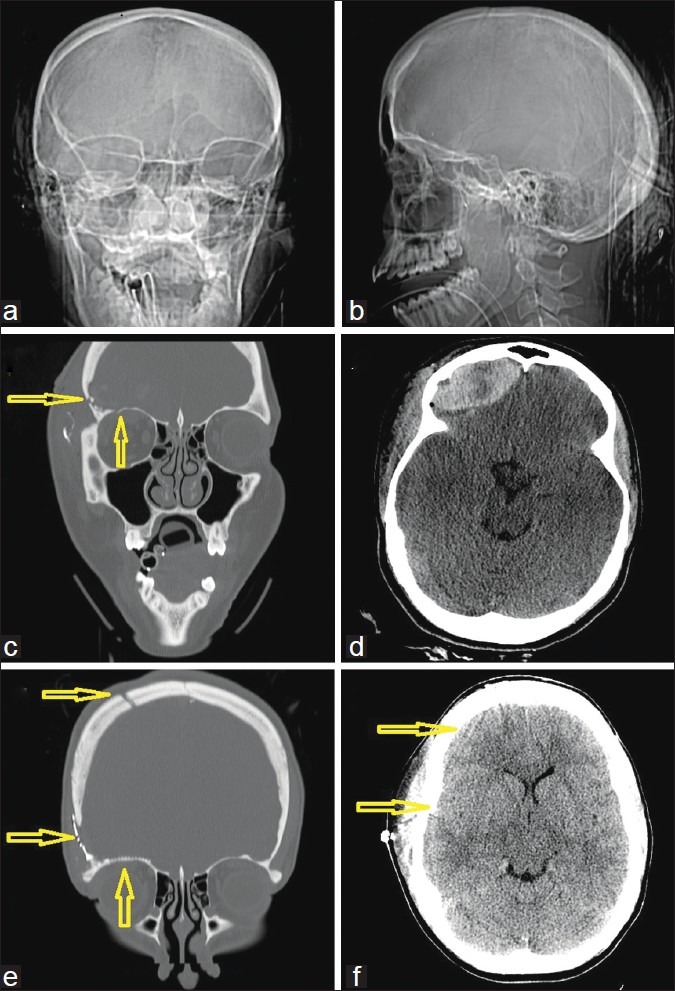
Results: Out of a total of 17 patients who went to the operating room (OR) for GSW to the head during this period, 4 cases with a GCS < 5 on admission were identified. All cases required a hemicraniectomy to alleviate cerebral swelling. Two cases presented with a unilaterally blown pupil due to raised intracranial pressure. The remaining 2 cases had equal and reactive pupils. One patient with a GCS of 3 and a significant bilateral pattern of parenchymal bullet injury was initially assessed in moribund status but rallied and received a delayed hemicraniectomy on day 7. Three out of 4 patients are functionally independent at 1-year follow-up. The fourth patient who received a delayed decompression remains wheelchair dependent.
Conclusion: Victims of GSWs can have good outcomes despite having a very poor admission GCS score and papillary abnormalities. Factors predicting good outcomes include the following: time from injury to surgical intervention of < 1 h; injury to noneloquent brain; and absence of injury to midbrain, brainstem, and major vessels.
Keywords: Decompressive hemicraniectomy; gunshot wounds; head; intracranial.
Figures
References
-
- Aldrich EF, Eisenberg HM, Saydjari C, Foulkes MA, Jane JA, Marshall LF, et al. Predictors of mortality in severely head-injured patients with civilian gunshot wounds: A report from the NIH Traumatic Coma Data Bank. Surg Neurol. 1992;38:418–23. - PubMed
-
- Benzel EC, Day WT, Kesterson L, Willis BK, Kessler CW, Modling D, et al. Civilian craniocerebral gunshot wounds. Neurosurgery. 1991;29:67–71. discussion 71-2. - PubMed
-
- Berlit P, Jaschke W, Tornow K. [Gunshot injuries of the skull.Computerized tomography findings and clinical course] Nervenarzt. 1987;58:300–4. - PubMed
-
- (CDC) CfDCaP. Nonfatal and fatal firearm-related injuries - United States. MMWR Morb Mortal Wkly Rep. 1999;48:1029–34. - PubMed
-
- Clark WC, Muhlbauer MS, Watridge CB, Ray MW. Analysis of 76 civilian craniocerebral gunshot wounds. J Neurosurg. 1986;65:9–14. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
