

The implementation of a community-based aerobic walking program for mild to moderate knee osteoarthritis (OA): a knowledge translation (KT) randomized controlled trial (RCT): Part I: The Uptake of the Ottawa Panel clinical practice guidelines (CPGs)
- PMID: 23061875
- PMCID: PMC3491047
- DOI: 10.1186/1471-2458-12-871
The implementation of a community-based aerobic walking program for mild to moderate knee osteoarthritis (OA): a knowledge translation (KT) randomized controlled trial (RCT): Part I: The Uptake of the Ottawa Panel clinical practice guidelines (CPGs)
Abstract
Background: The implementation of evidence based clinical practice guidelines on self-management interventions to patients with chronic diseases is a complex process. A multifaceted strategy may offer an effective knowledge translation (KT) intervention to promote knowledge uptake and improve adherence in an effective walking program based on the Ottawa Panel Evidence Based Clinical Practice Guidelines among individuals with moderate osteoarthritis (OA).
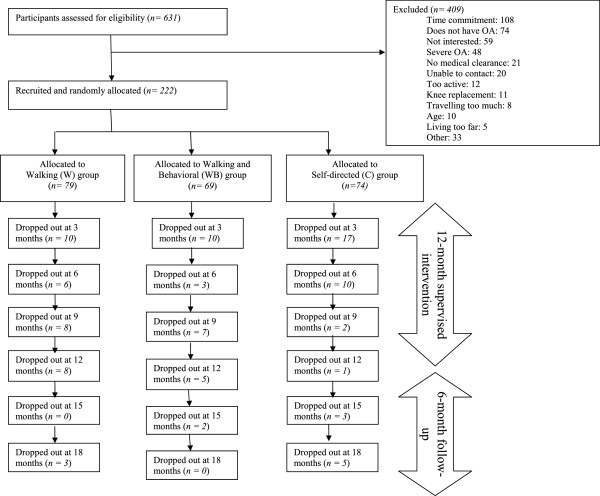
Methods: A single-blind, randomized control trial was conducted. Patients with mild to moderate (OA) of the knee (n=222) were randomized to one of three KT groups: 1) Walking and Behavioural intervention (WB) (18 males, 57 females) which included the supervised community-based aerobic walking program combined with a behavioural intervention and an educational pamphlet on the benefits of walking for OA; 2) Walking intervention (W) (24 males, 57 females) wherein participants only received the supervised community-based aerobic walking program intervention and the educational pamphlet; 3) Self-directed control (C) (32 males, 52 females) wherein participants only received the educational pamphlet. One-way analyses of variance were used to test for differences in quality of life, adherence, confidence, and clinical outcomes among the study groups at each 3 month assessment during the 12-month intervention period and 6-month follow-up period.
Results: Short-term program adherence was greater in WB compared to C (p<0.012) after 3 months. No statistical significance (p> 0.05) was observed for long-term adherence (6 to 12 months), and total adherence between the three groups. The three knowledge translation strategies demonstrated equivalent long-term results for the implementation of a walking program for older individuals with moderate OA. Lower dropout rates as well as higher retention rates were observed for WB at 12 and 18 months.
Conclusion: The additional knowledge translation behavioural component facilitated the implementation of clinical practice guidelines on walking over a short-term period. More studies are needed to improve the long-term walking adherence or longer guidelines uptake on walking among participants with OA. Particular attention should be taken into account related to patient's characteristic and preference. OA can be managed through the implementation of a walking program based on clinical practice guidelines in existing community-based walking clubs as well as at home with the minimal support of an exercise therapist or a trained volunteer.
Trial registration: Current Controlled Trials IRSCTNO9193542.
Figures
References
-
- Jordan JM, Helmick CG, Renner JB, Luta G, Dragomir AD, Woodard J, Fang F, Schwartz TA, Abbate LM, Callahan LF, Kalsbeek WD, Hochberg MC. Prevalence of knee symptoms and radiographic and symptomatic knee osteoarthritis in African Americans and Caucasians: the Johnson Country Osteoarthritis Project. J Rheumatol. 2007;34(1):172–180. - PubMed
-
- Grotle M, Hagen KB, Natvig B, Dahl FA, Kvien TK. Prevalence and burden of osteoarthritis: results from a population survey in Norway. J Rheumatol. 2008;35(4):677–684. - PubMed
-
- Vetter NJ. Effect of an aging population on service use. Reviews in Clinical Gerontology. 2005;15:55–62. doi: 10.1017/S0959259805001693. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
