

Geographic variation in Medicare spending and mortality for diabetic patients with foot ulcers and amputations
- PMID: 23062327
- PMCID: PMC3673572
- DOI: 10.1016/j.jdiacomp.2012.09.003
Geographic variation in Medicare spending and mortality for diabetic patients with foot ulcers and amputations
Abstract
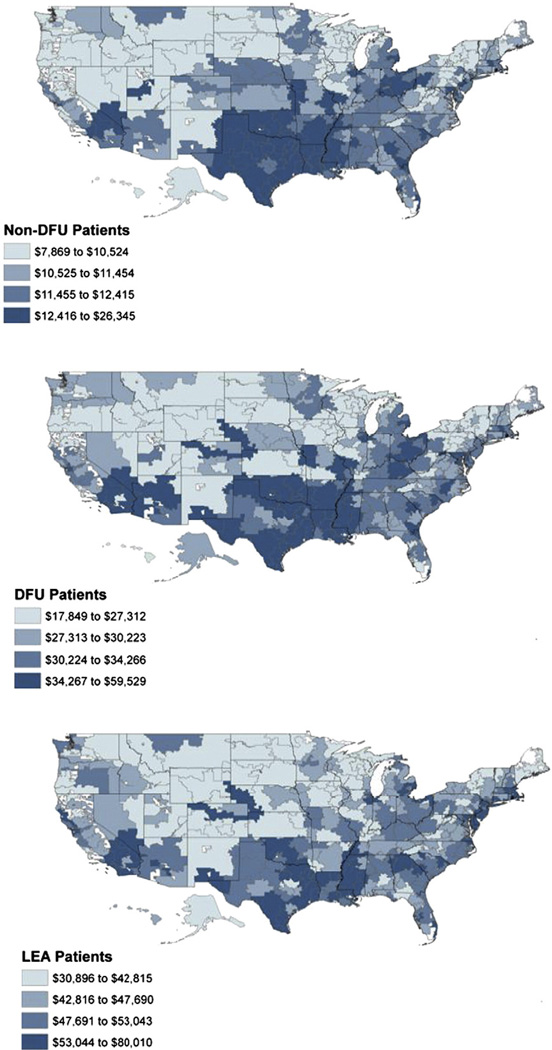
Aims: The purpose of this study was to identify the presence or absence of geographic variation in Medicare spending and mortality rates for diabetic patients with foot ulcers (DFU) and lower extremity amputations (LEA).
Methods: Diabetic beneficiaries with foot ulcers (n=682,887) and lower extremity amputations (n=151,752) were enrolled in Medicare Parts A and B during the calendar year 2007. We used ordinary least squares (OLS) regression to explain geographic variation in per capita Medicare spending and one-year mortality rates.
Results: Health care spending and mortality rates varied considerably across the nation for our two patient cohorts. However, higher spending was not associated with a statistically significant reduction in one-year patient mortality (P=.12 for DFU, P=.20 for LEA). Macrovascular complications for amputees were more common in parts of the country with higher mortality rates (P<.001), but this association was not observed for our foot ulcer cohort (P=.12). In contrast, macrovascular complications were associated with increased per capita spending for beneficiaries with foot ulcers (P=.01). Rates of hospital admission were also associated with higher per capita spending and increased mortality rates for individuals with foot ulcers (P<.001 for health spending and mortality) and lower extremity amputations (P<.001 for health spending, P=.01 for mortality).
Conclusions: Geographic variation in Medicare spending and mortality rates for diabetic patients with foot ulcers and amputations is associated with regional differences in the utilization of inpatient services and the prevalence of macrovascular complications.
Copyright © 2013. Published by Elsevier Inc.
Figures
References
-
- American Diabetes Association. Economic costs of diabetes in the U.S. In 2007. Diabetes Care. 2008;31:596–615. - PubMed
-
- Aulivola B, Hile CN, Hamdan AD, et al. Major lower extremity amputation: outcome of a modern series. Archives of Surgery. 2004;139:395–399. [discussion 9] - PubMed
-
- Fisher ES, Wennberg DE, Stukel TA, Gottlieb DJ, Lucas FL, Pinder EL. The implications of regional variations in Medicare spending. Part 1: the content, quality, and accessibility of care. Annals of Internal Medicine. 2003;138:273–287. - PubMed
-
- Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. New England Journal of Medicine. 1998;339:229–234. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
