

Can existing drugs approved for other indications retard renal function decline in patients with type 1 diabetes and nephropathy?
- PMID: 23062984
- PMCID: PMC3474984
- DOI: 10.1016/j.semnephrol.2012.07.006
Can existing drugs approved for other indications retard renal function decline in patients with type 1 diabetes and nephropathy?
Abstract
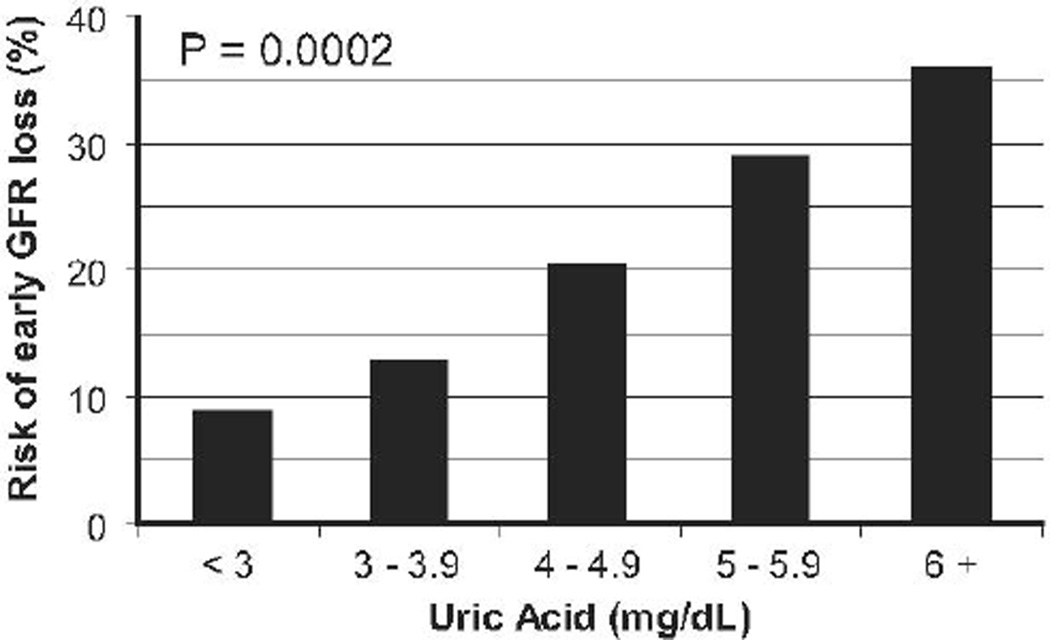
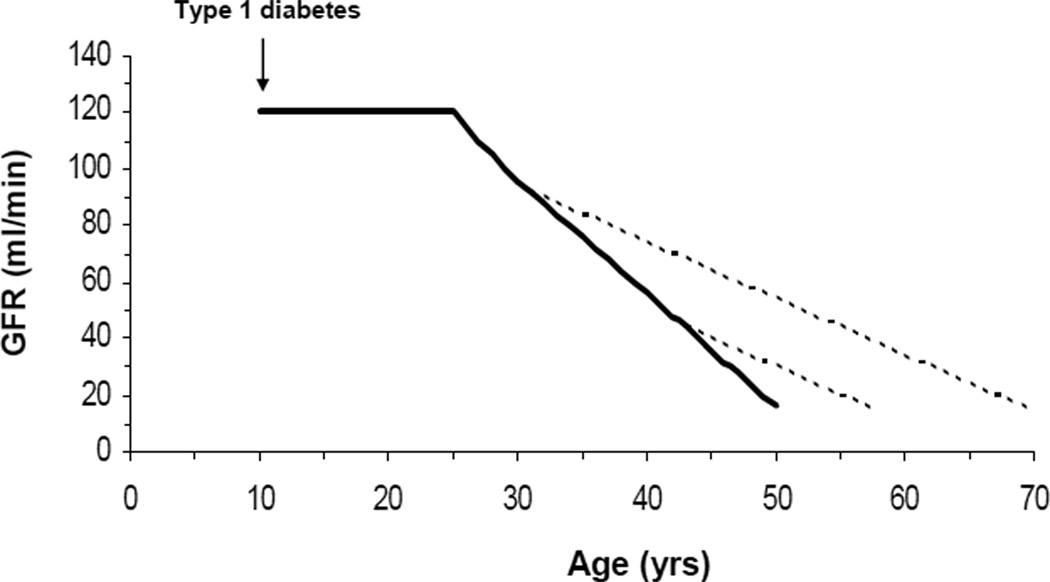
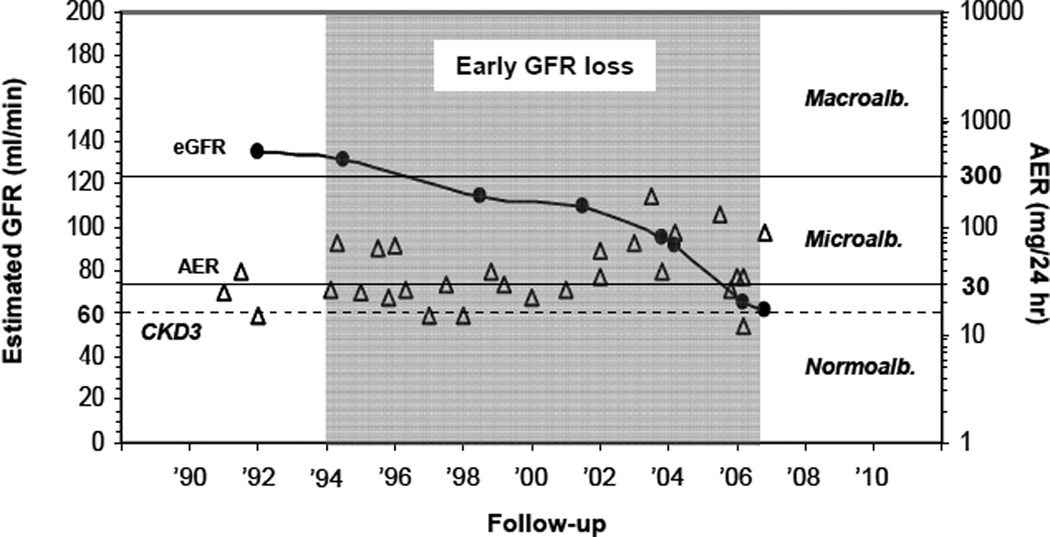
Mounting evidence from human, animal, and in vitro studies indicates that existing drugs, developed to treat other disorders, also might be effective in preventing or slowing the progression of diabetic nephropathy to end-stage renal disease. Examples of such drugs include the urate-lowering agent allopurinol, the anti-tumor necrosis factor agents etanercept and infliximab, and the immunomodulating drug abatacept. Because some of these medications are already on the market and have been used for a number of years for other indications, they can be tested immediately in human beings for a beneficial effect on renal function in diabetes. Special emphasis should be placed on evaluating the use of these drugs early in the course of diabetic nephropathy when renal damage is most likely to be reversible and interventions can yield the greatest delay to end-stage renal disease.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
References
-
- Krolewski AS, Warram JH. Epidemiology of late complications of diabetes: A basis for the development and evaluation of preventive program. In: Kahn CR, Weir GC, King GL, Jacobson AM, Moses AC, Smith RJ, editors. Joslin's Diabetes Mellitus. New York: Lippincott, Williams & Wilkins; 2005.
-
- U S Renal Data System. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2010. USRDS 2010 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
