

Relative mitochondrial priming of myeloblasts and normal HSCs determines chemotherapeutic success in AML
- PMID: 23063124
- PMCID: PMC3534747
- DOI: 10.1016/j.cell.2012.08.038
Relative mitochondrial priming of myeloblasts and normal HSCs determines chemotherapeutic success in AML
Abstract
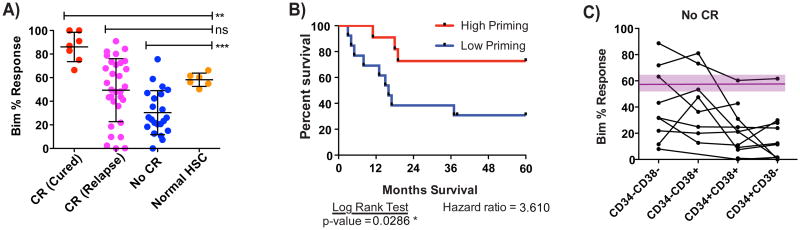
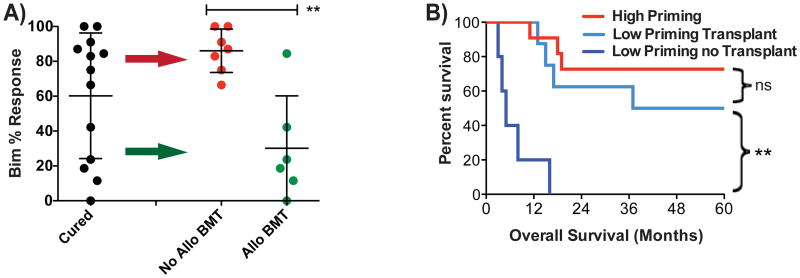
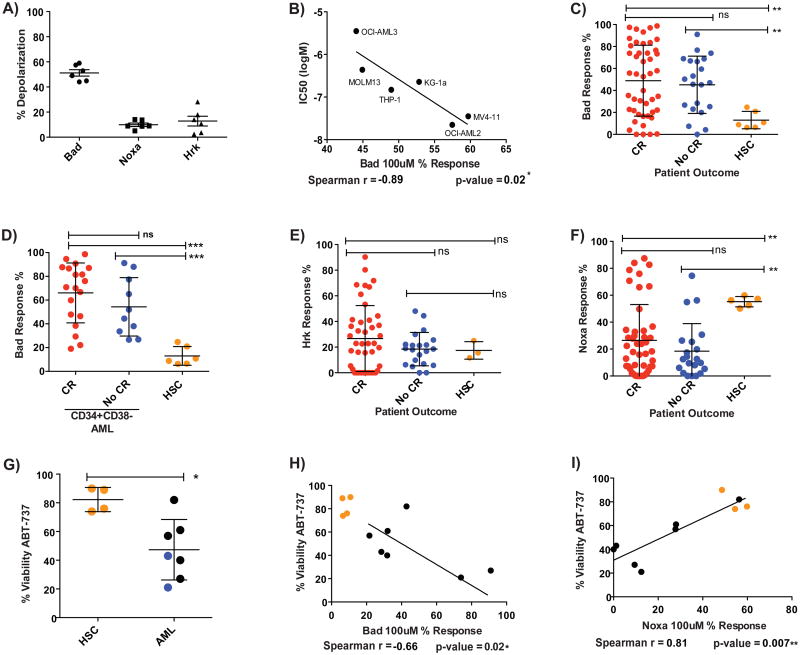
Despite decades of successful use of cytotoxic chemotherapy in acute myelogenous leukemia (AML), the biological basis for its differential success among individuals and for the existence of a therapeutic index has remained obscure. Rather than taking a genetic approach favored by many, we took a functional approach to ask how differential mitochondrial readiness for apoptosis ("priming") might explain individual variation in clinical behavior. We found that mitochondrial priming measured by BH3 profiling was a determinant of initial response to induction chemotherapy, relapse after remission, and requirement for allogeneic bone marrow transplantation. Differential priming between malignant myeloblasts and normal hematopoietic stem cells supports a mitochondrial basis to the therapeutic index for chemotherapy. BH3 profiling identified BCL-2 inhibition as a targeted strategy likely to have a useful therapeutic index. BH3 profiling refines predictive information provided by conventional biomarkers currently in use and thus may itself have utility as a clinical predictive biomarker. PAPERCLIP:
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
References
-
- Certo M, Del Gaizo Moore V, Nishino M, Wei G, Korsmeyer S, Armstrong SA, Letai A. Mitochondria primed by death signals determine cellular addiction to antiapoptotic BCL-2 family members. Cancer Cell. 2006;9:351–365. - PubMed
-
- Chen L, Willis SN, Wei A, Smith BJ, Fletcher JI, Hinds MG, Colman PM, Day CL, Adams JM, Huang DC. Differential targeting of prosurvival Bcl-2 proteins by their BH3-only ligands allows complementary apoptotic function. Mol Cell. 2005;17:393–403. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
