

Calculating the risk benefit equation for aggressive treatment of non-convulsive status epilepticus
- PMID: 23065689
- PMCID: PMC3767472
- DOI: 10.1007/s12028-012-9785-y
Calculating the risk benefit equation for aggressive treatment of non-convulsive status epilepticus
Abstract
Objective: To address the question: does non-convulsive status epilepticus warrant the same aggressive treatment as convulsive status epilepticus?
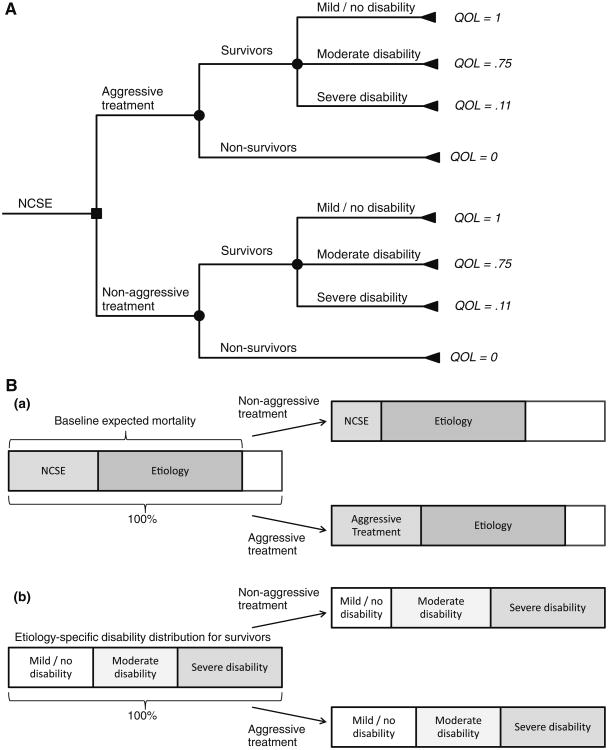
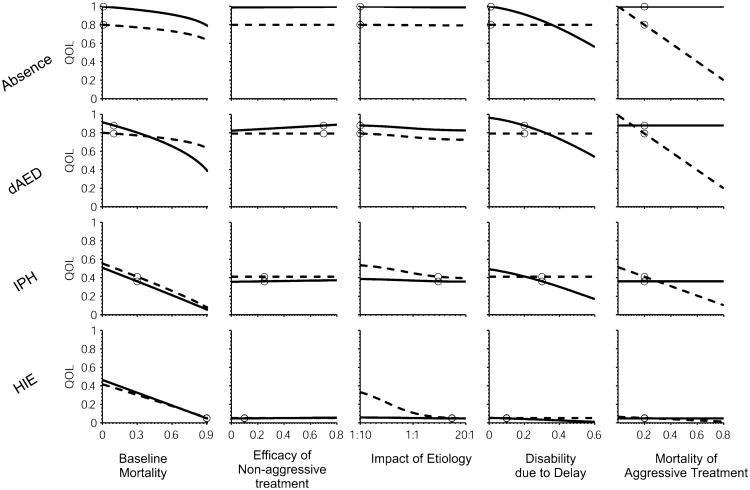
Methods: We used a decision model to evaluate the risks and benefits of treating non-convulsive status epilepticus with intravenous anesthetics and ICU-level aggressive care. We investigated how the decision to use aggressive versus non-aggressive management for non-convulsive status epilepticus impacts expected patient outcome for four etiologies: absence epilepsy, discontinued antiepileptic drugs, intraparenchymal hemorrhage, and hypoxic ischemic encephalopathy. Each etiology was defined by distinct values for five key parameters: baseline mortality rate of the inciting etiology; efficacy of non-aggressive treatment in gaining control of seizures; the relative contribution of seizures to overall mortality; the degree of excess disability expected in the case of delayed seizure control; and the mortality risk of aggressive treatment.
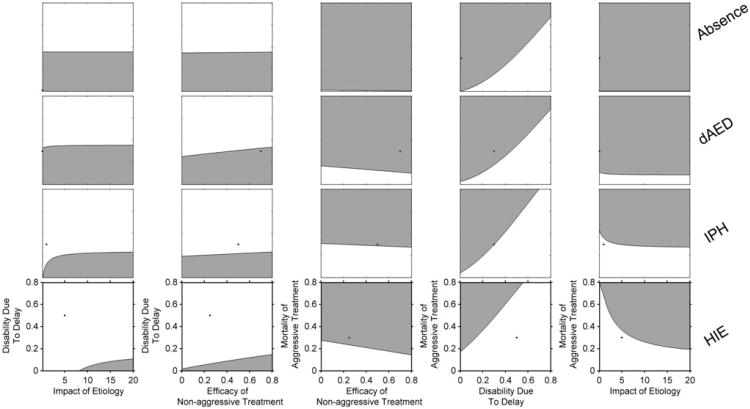
Results: Non-aggressive treatment was favored for etiologies with low morbidity and mortality such as absence epilepsy and discontinued antiepileptic drugs. The risk of aggressive treatment was only warranted in etiologies where there was significant risk of seizure-induced neurologic damage. In the case of post-anoxic status epilepticus, expected outcomes were poor regardless of the treatment chosen. The favored strategy in each case was determined by strong interactions of all five model parameters.
Conclusions: Determination of the optimal management approach to non-convulsive status epilepticus is complex and is ultimately determined by the inciting etiology.
Figures
Similar articles
-
Predictors of Outcome of Convulsive Status Epilepticus Among an Egyptian Pediatric Tertiary Hospital.J Child Neurol. 2015 Nov;30(13):1736-42. doi: 10.1177/0883073815579706. Epub 2015 Apr 20. J Child Neurol. 2015. PMID: 25895912
-
Pre-hospital and emergency department treatment of convulsive status epilepticus in adults: an evidence synthesis.Health Technol Assess. 2022 Mar;26(20):1-76. doi: 10.3310/RSVK2062. Health Technol Assess. 2022. PMID: 35333156 Free PMC article.
-
Functional outcome after convulsive status epilepticus.Crit Care Med. 2010 Dec;38(12):2295-303. doi: 10.1097/CCM.0b013e3181f859a6. Crit Care Med. 2010. PMID: 20890201
-
Third-line antiepileptic therapy and outcome in status epilepticus: the impact of vasopressor use and prolonged mechanical ventilation.Crit Care Med. 2012 Sep;40(9):2677-84. doi: 10.1097/CCM.0b013e3182591ff1. Crit Care Med. 2012. PMID: 22732291
-
Current Trends in Treatment of Status Epilepticus and Refractory Status Epilepticus.Semin Neurol. 2015 Dec;35(6):621-8. doi: 10.1055/s-0035-1564304. Epub 2015 Nov 23. Semin Neurol. 2015. PMID: 26595862 Review.
Cited by
-
Anesthetic drugs in status epilepticus: risk or rescue? A 6-year cohort study.Neurology. 2014 Feb 25;82(8):656-64. doi: 10.1212/WNL.0000000000000009. Epub 2013 Dec 6. Neurology. 2014. PMID: 24319039 Free PMC article.
-
What's new in status epilepticus?Intensive Care Med. 2014 Sep;40(9):1359-62. doi: 10.1007/s00134-014-3363-z. Epub 2014 Jun 13. Intensive Care Med. 2014. PMID: 24923581 No abstract available.
-
International consensus recommendations for management of New Onset Refractory Status Epilepticus (NORSE) incl. Febrile Infection-Related Epilepsy Syndrome (FIRES): Statements and Supporting Evidence.Epilepsia. 2022 Aug 23;63(11):2840-64. doi: 10.1111/epi.17397. Online ahead of print. Epilepsia. 2022. PMID: 35997591 Free PMC article.
-
Nonconvulsive seizures and nonconvulsive status epilepticus in the neuro ICU should or should not be treated aggressively: A debate.Clin Neurophysiol Pract. 2019 Aug 9;4:170-177. doi: 10.1016/j.cnp.2019.07.001. eCollection 2019. Clin Neurophysiol Pract. 2019. PMID: 31886441 Free PMC article. Review.
-
Anesthetics and Outcome in Status Epilepticus: A Matched Two-Center Cohort Study.CNS Drugs. 2017 Jan;31(1):65-74. doi: 10.1007/s40263-016-0389-5. CNS Drugs. 2017. PMID: 27896706
References
-
- Kaplan PW. Assessing the outcomes in patients with nonconvulsive status epilepticus: nonconvulsive status epilepticus is underdiagnosed, potentially overtreated, and confounded by comorbidity. J Clin Neurophysiol. 1999;16(4):341–52. discussion 353. - PubMed
-
- Chong DJ, Hirsch LJ. Which EEG patterns warrant treatment in the critically ill? Reviewing the evidence for treatment of periodic epileptiform discharges and related patterns. J Clin Neurophysiol. 2005;22(2):79–91. - PubMed
-
- Young GB, Jordan KG. Do nonconvulsive seizures damage the brain?–Yes. Arch Neurol. 1998;55(1):117. - PubMed
-
- Aminoff MJ. Do nonconvulsive seizures damage the brain?–No. Arch Neurol. 1998;55(1):119–20. - PubMed
-
- Kaplan PW. No, some types of nonconvulsive status epilepticus cause little permanent neurologic sequelae (or: “the cure may be worse than the disease”) Neurophysiol Clin. 2000;30(6):377–82. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
