

Clinical outcome and predictors of survival after TIPS insertion in patients with liver cirrhosis
- PMID: 23066315
- PMCID: PMC3468853
- DOI: 10.3748/wjg.v18.i37.5211
Clinical outcome and predictors of survival after TIPS insertion in patients with liver cirrhosis
Abstract
Aim: To determine the clinical outcome and predictors of survival after transjugular intrahepatic portosystemic stent shunt (TIPS) implantation in cirrhotic patients.
Methods: Eighty-one patients with liver cirrhosis and consequential portal hypertension had TIPS implantation (bare metal) for either refractory ascites (RA) (n = 27) or variceal bleeding (VB) (n = 54). Endpoints for the study were: technical success, stent occlusion and stent stenosis, rebleeding, RA and mortality. Clinical records of patients were collected and analysed. Baseline characteristics [e.g., age, sex, CHILD score and the model for end-stage liver disease score (MELD score), underlying disease] were retrieved. The Kaplan-Meier method was employed to calculate survival from the time of TIPS implantation and comparisons were made by log rank test. A multivariate analysis of factors influencing survival was carried out using the Cox proportional hazards regression model. Results were expressed as medians and ranges. Comparisons between groups were performed by using the Mann-Whitney U-test and the χ2 test as appropriate.
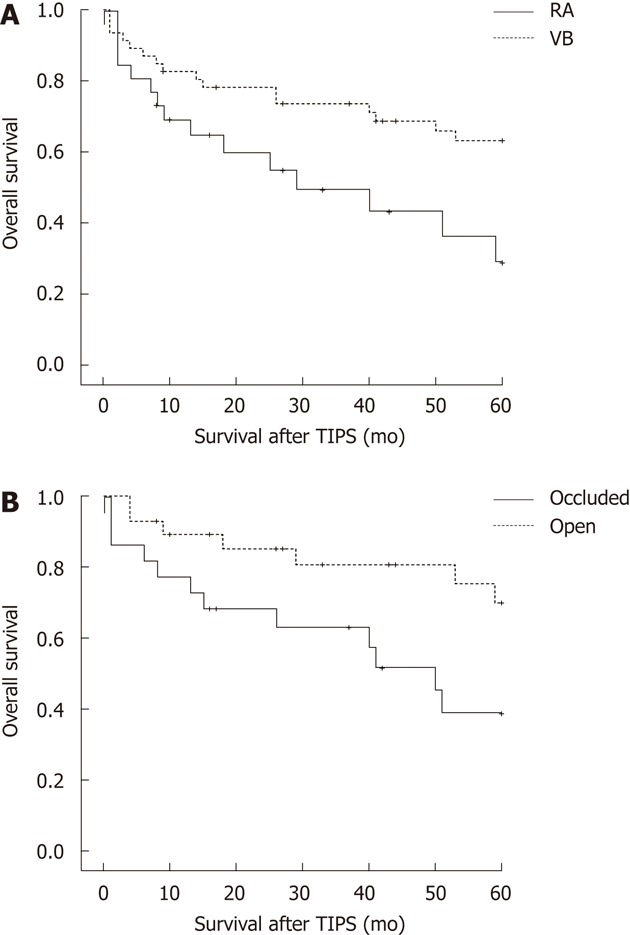
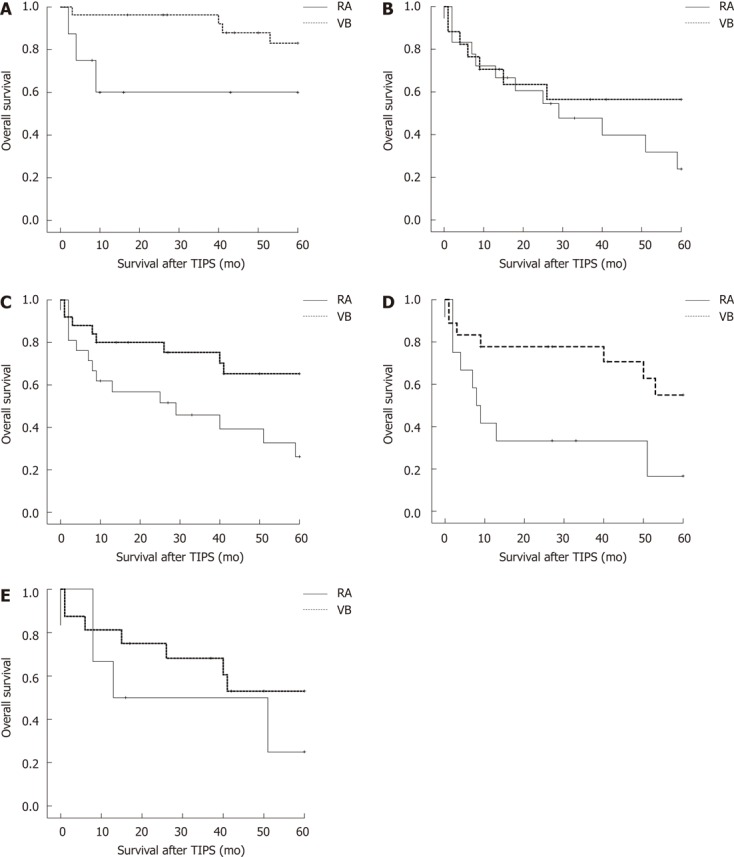
Results: No difference could be seen in terms of age, sex, underlying disease or degree of portal pressure gradient (PPG) reduction between the ascites and the bleeding group. The PPG significantly decreased from 23.4 ± 5.3 mmHg (VB) vs. 22.1 ± 5.5 mmHg (RA) before TIPS to 11.8 ± 4.0 vs. 11.7 ± 4.2 after TIPS implantation (P = 0.001 within each group). There was a tendency towards more patients with stage CHILD A in the bleeding group compared to the ascites group (24 vs 6, P = 0.052). The median survival for the ascites group was 29 mo compared to > 60 mo for the bleeding group (P = 0.009). The number of radiological controls for stent patency was 6.3 for bleeders and 3.8 for ascites patients (P = 0.029). Kaplan-Meier calculation indicated that stent occlusion at first control (P = 0.027), ascites prior to TIPS implantation (P = 0.009), CHILD stage (P = 0.013), MELD score (P = 0.001) and those patients not having undergone liver transplantation (P = 0.024) were significant predictors of survival. In the Cox regression model, stent occlusion (P = 0.022), RA (P = 0.043), CHILD stage (P = 0.015) and MELD score (P = 0.004) turned out to be independent prognostic factors of survival. The anticoagulation management (P = 0.097), the porto-systemic pressure gradient (P = 0.460) and rebleeding episodes (P = 0.765) had no significant effect on the overall survival.
Conclusion: RA, stent occlusion, initial CHILD stage and MELD score are independent predictors of survival in patients with TIPS, speaking for a close follow-up in these circumstances.
Keywords: Ascites; Gastrointestinal hemorrhage; Liver cirrhosis; Transjugular intrahepatic portosystemic stent shunt; Treatment outcome.
Figures
Similar articles
-
Long-term clinical outcomes in patients with viral hepatitis related liver cirrhosis after transjugular intrahepatic portosystemic shunt treatment.Virol J. 2018 Oct 1;15(1):151. doi: 10.1186/s12985-018-1067-7. Virol J. 2018. PMID: 30285813 Free PMC article.
-
Long-term clinical outcome and survival predictors in patients with cirrhosis after 10-mm-covered transjugular intrahepatic portosystemic shunt.Gastroenterol Hepatol. 2021 Nov;44(9):620-627. doi: 10.1016/j.gastrohep.2020.10.018. Epub 2020 Nov 26. Gastroenterol Hepatol. 2021. PMID: 33249114 English, Spanish.
-
Transjugular Intrahepatic Porto-Systemic Shunt in Patients with Liver Cirrhosis and Model for End-Stage Liver Disease ≥15.Dig Dis Sci. 2017 Feb;62(2):534-542. doi: 10.1007/s10620-016-4185-3. Epub 2016 May 6. Dig Dis Sci. 2017. PMID: 27154510
-
The role of transjugular intrahepatic portosystemic shunt (TIPS) in the management of portal hypertension.J Clin Gastroenterol. 2007 Nov-Dec;41 Suppl 3:S344-51. doi: 10.1097/MCG.0b013e318157e500. J Clin Gastroenterol. 2007. PMID: 17975487 Review.
-
Outcome of Children with Transjugular Intrahepatic Portosystemic Shunt: A Meta-Analysis of Individual Patient Data.Cardiovasc Intervent Radiol. 2023 Sep;46(9):1203-1213. doi: 10.1007/s00270-023-03520-z. Epub 2023 Aug 2. Cardiovasc Intervent Radiol. 2023. PMID: 37532945 Free PMC article. Review.
Cited by
-
Elective Transjugular Intrahepatic Portosystemic Shunt Using Viatorr Stent-Grafts: A Single-Center Experience from China.J Belg Soc Radiol. 2022 Jun 29;106(1):62. doi: 10.5334/jbsr.2741. eCollection 2022. J Belg Soc Radiol. 2022. PMID: 35854822 Free PMC article.
-
Volumetric blood flow in transjugular intrahepatic portosystemic shunt revision using 3-dimensional Doppler sonography.J Ultrasound Med. 2015 Feb;34(2):257-66. doi: 10.7863/ultra.34.2.257. J Ultrasound Med. 2015. PMID: 25614399 Free PMC article. Clinical Trial.
-
Long-term clinical outcomes in patients with viral hepatitis related liver cirrhosis after transjugular intrahepatic portosystemic shunt treatment.Virol J. 2018 Oct 1;15(1):151. doi: 10.1186/s12985-018-1067-7. Virol J. 2018. PMID: 30285813 Free PMC article.
-
Predicting death or recurrence of portal hypertension symptoms after TIPS procedures.Eur Radiol. 2022 May;32(5):3346-3357. doi: 10.1007/s00330-021-08437-0. Epub 2022 Jan 11. Eur Radiol. 2022. PMID: 35015124
-
Nationwide trends and predictors of inpatient mortality in 83884 transjugular intrahepatic portosystemic shunt.World J Gastroenterol. 2016 Jul 7;22(25):5780-9. doi: 10.3748/wjg.v22.i25.5780. World J Gastroenterol. 2016. PMID: 27433091 Free PMC article.
References
-
- de Franchis R, Dell’Era A, Iannuzzi F. Diagnosis and treatment of portal hypertension. Dig Liver Dis. 2004;36:787–798. - PubMed
-
- Garcia-Tsao G. Current management of the complications of cirrhosis and portal hypertension: variceal hemorrhage, ascites, and spontaneous bacterial peritonitis. Gastroenterology. 2001;120:726–748. - PubMed
-
- Ginès P, Cárdenas A, Arroyo V, Rodés J. Management of cirrhosis and ascites. N Engl J Med. 2004;350:1646–1654. - PubMed
-
- Ginès P, Guevara M, Arroyo V, Rodés J. Hepatorenal syndrome. Lancet. 2003;362:1819–1827. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
